
.jpg)
Case Series/Study
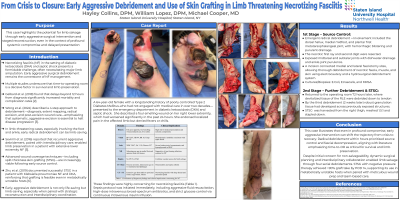
Purpose: Necrotizing fasciitis (NF) in the setting of diabetic ketoacidosis (DKA) and septic shock presents a formidable challenge, often necessitating major limb amputation. This case highlights the potential for limb salvage through early aggressive surgical intervention and staged reconstruction, even amidst profound systemic compromise and delayed presentation.
Background: NF is a rapidly progressive soft tissue infection with high morbidity and mortality, particularly in patients with diabetes. Mortality rates range from 25–35%, and early diagnosis is frequently missed. Diabetic patients are especially vulnerable due to immunocompromise, vascular disease, and delayed care. Literature emphasizes prompt surgical debridement, interdisciplinary coordination, and advanced wound coverage techniques—including dermal regeneration matrices and split‑thickness skin grafting—as viable strategies for limb salvage.
Case Presentation: A 64‑year‑old female with poorly controlled Type 2 Diabetes Mellitus, who had not seen a physician in over two decades, presented in DKA and septic shock. She reported a foul‑smelling right foot wound with blistering that worsened over 24 hours. Labs revealed leukocytosis (38.47), hyponatremia (119), and hyperglycemia (557).
Surgical Procedure:
Stage 1 – Source Control: Emergent radical debridement was performed with plastic surgery. Necrotic first ray and second digit were resected. Fasciotomies allowed thorough debridement of necrotic fascia, muscle, and skin using electrocautery and hydrosurgical techniques.
Stage 2 – Reconstruction: Two weeks later, devitalized tissue was further debrided, and a split‑thickness skin graft harvested from the right thigh was meshed and applied to a 10 × 20 cm wound bed. Negative pressure therapy and compressive dressings supported graft take.