Introduction: Limb preservation in diabetic and neuropathic patients requires early recognition of vascular compromise, infection, and structural deformity before they progress to limb-threatening pathology. Major lower-extremity amputation carries a 5-year mortality of 40–70%, underscoring the need for proactive strategies that prevent ulcer progression and limb loss. VISTA—Vascular evaluation, Infection control, Surgical correction, Technologies & therapies, and Amputation prevention—provides a structured pathway that identifies limb-threatening risk and guides timely intervention. This practice innovation project evaluates real-world implementation of VISTA across a 60-case surgical cohort involving forefoot, midfoot, rearfoot, and Charcot reconstruction procedures.
Methods: A three-year retrospective analysis was performed on 60 consecutive VISTA-guided surgical cases from 2021–2024. Vascular evaluation confirmed adequate perfusion or prompted revascularization before surgery. Infection control included culture-directed antibiotics, sharp debridement, and antibiotic bone void fillers when osteomyelitis or deep infection was present. Structural correction was performed in all cases to redistribute pathological pressure contributing to current or potential ulceration. Technologies such as negative pressure wound therapy, advanced dressings, digital imaging, and external fixation were used when indicated. Surgical categories included 44 forefoot, 11 midfoot (including 2 Charcot), and 5 rearfoot procedures, with 29 preventative surgeries, 3 preventative cases with previously healed ulcers, and 28 ulcer- presenting cases. Outcomes assessed included healing progression and limb preservation.
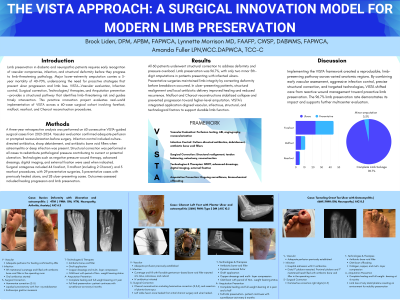
Results: All 60 patients underwent structural correction to address deformity and pressure overload. Limb preservation was 96.7%, with only two minor 5th-digit amputations in patients presenting with infected ulcers. Preventative surgeries maintained limb integrity by correcting deformity before breakdown occurred. In ulcer-presenting patients, structural realignment and local antibiotic delivery improved healing and reduced recurrence. Midfoot and Charcot reconstructions stabilized collapse and prevented progression toward higher-level amputation. VISTA’s integrated application aligned vascular, infectious, structural, and technological factors to support durable limb function.
Discussion: Implementing the VISTA framework created a reproducible, limb-preserving pathway across varied anatomic regions. By combining early vascular assessment, aggressive infection control, precise structural correction, and targeted technologies, VISTA shifted care from reactive wound management toward proactive limb preservation. The 96.7% limb preservation rate demonstrates its impact and supports further multicenter evaluation.

.jpg)