(CS-134) Applying Fluorescence Imaging in Routine Wound Assessment: Practical Lessons from Two Cases
Friday, April 10, 2026
Mario Aurelio Martínez Jiménez, MD,PhD; Heba Tallah Mohammed, MD,PhD – Swift Medical Inc.; Basnama Ayaz, PhD; Samia Rahman, MD; Robert D. J. Fraser, BScN,MN – Swift Medical Inc.
Introduction: Clinicians often use visual inspection and experience to confirm the presence of bacteria;however, the early signs are usually subtle. Fluorescence (FL) imaging gives a real-time insight into bacterial activitywhen the clinical findings are uncertain. Having this information instantly can influence how quickly a clinician can advance treatment or address bacterial burden before moving ahead.
Methods: Point-of-care FL imaging was used at an outpatient clinic.FL patterns were interpreted with visual findings to guide immediate, case-specific treatment decisions.Two cases are presented to show how FL imaging supported clinical decision-making.
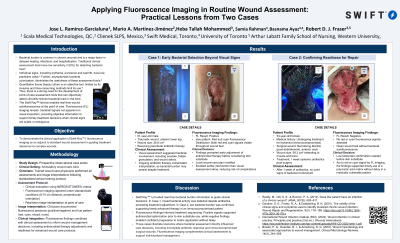
Results: Case 1: A female patientaged 54 in treatment for leukemiapresented with a complicated dental abscess that developed into a large anterior-neck necrotizing fasciitis. After debriding the infected tissue, a 58.3 cm² woundextending to muscle and osseous planes was left behind. Despite such large size and morphology, no overt signs of bacterial involvement were evident visually in this wound bed after 1 week of antibiotic treatment. Confirmation of a low-bioburden environment is important before proceeding to add skin substitute for repair.The FL scan did not display red or cyan fluorescence, which was consistent with the visual cues indicating the absence of bacterial load at that time. This result supported the clinical team’s decision to move ahead with their treatment plan usingpoly-tactic acid matrix and prevented unnecessary delay for this medically vulnerable patient. Case 2: A 61-year-old male had a traumatic wound measured 26.8 cm² on the anterior lower leg. Although he received parenteral antibiotics, FL images showed both red and cyan fluorescence signals that suggest mixed bacterial activity, thus enabling the adjustment of antibiotics before considering skin substitute. These FL scans were utilized by the clinician to start a timely antimicrobial therapy and adjust the local wound-care plan. This occurred earlier than one might expect with surveillance based on visible changes and decreased the likelihood of subsequent complications, supporting earlier active management.
Discussion: These cases illustrate the potential of point-of-care FL imaging to provide immediate, objective information about bacterial presence and supplement standard-of-care wound assessment, improve decisions and overall outcomes

.jpg)