
.jpg)
Clinical Research
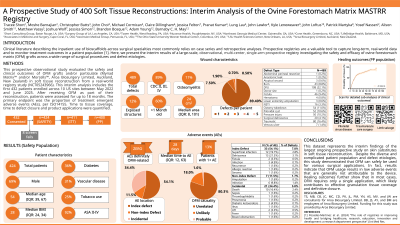
A total of 432 patients were enrolled, with n=7 screen failures. Of the n=425 Safety population (SP), n=14 were lost to follow-up (LTFU) immediately after index procedure, leaving n=411 in the Intent to Treat (ITT) population; n=400 completed ≥ 14 days of follow-up (Per Protocol population). Fifty-three SP patients reported ≥1 AEs (12.5%), and there were a total of 63 unique AEs reported. The most common AEs were dehiscence (~3.1%), superficial infection (~2.8%), infection (~2.4%) or death (~2.4%). Most AEs were concluded to be unrelated (80.6%) or unlikely (17.7%) to be related to the OFM graft. A single (~0.2%) AE, ‘allergic reaction’ was concluded to ‘probably’ be related to the OFM graft, though this could not be confirmed via pathology. There were no reported incidents of graft loss.
PP patients (n=400) had a median of one defect per patient (range; 1, 5) giving a total of n=464 defects. This included many defect types including burns (8.6%), DFU (22.1%), fistulae (9.5%), NSTI (2.9%), ostomy takedowns (10.9%), pilonidal sinus (10.7%), pressure injury (9.1%), surgical dehiscence (4.0%) and defects resulting from trauma (16.4%). Sub-group analysis of efficacy outcomes has shown the time to tissue coverage or fill of 2-4 weeks, depending on the extent of the defect and patient factors, and is consistent with prior published studies.
Discussion: This interim analysis demonstrates that OFM grafts have a low complication rate and are clinically effective.