
.jpg)
Case Series/Study
Purpura fulminans is a rare, life-threatening disorder marked by rapidly evolving cutaneous necrosis, microvascular thrombosis, and disseminated intravascular coagulation (DIC), often triggered by severe sepsis.1 Our case involves a 37-year-old woman with a complex medical and obstetric history, who developed purpura fulminans in the setting of E. coli bacteremia and multiorgan failure. Her prior surgical history (Whipple procedure) and obstetric complications (focal placenta accreta, manual placental extraction after normal spontaneous vaginal delivery at 36 weeks) further complicated her presentation. Following onset of lower-extremity swelling, sepsis, altered mental status, dialysis-dependent renal failure, and ventilatory support, she was transferred to a medical intensive care unit. Once necrotic skin lesions consistent with purpura fulminans appeared, advanced wound-care management was initiated.
Methods:
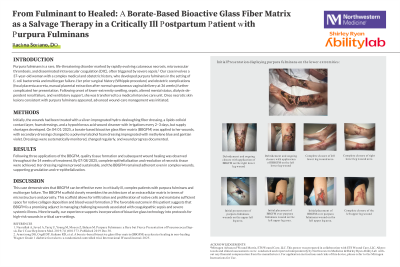
Initially, the wounds had been treated with a silver-impregnated hydro-desloughing fiber dressing, a lipido-colloid contact layer, foam dressings, and a hypochlorous acid wound cleanser with irrigations every 2–3 days, but supply shortages developed. On 04/01/2025, a borate-based bioactive glass fiber matrix (BBGFM) was applied to her wounds, with secondary dressings changed to a polyvinyl alcohol foam dressing impregnated with methylene blue and gentian violet. Dressings were systematically monitored, changed regularly, and wound progress documented.
Results: Following three applications of the BBGFM, quality tissue formation and subsequent wound healing was observed throughout the 14 weeks of treatment. By 07/08/2025, complete epithelialization and resolution of necrotic tissue were achieved. Her dressing regimen proved sustainable, and the BBGFM remained adherent even in complex wounds, supporting granulation and re-epithelialization
Discussion:
This case demonstrates that BBGFM can be effective even in critically ill, complex patients with purpura fulminans and multiorgan failure. The BBGFM scaffold closely resembles the architecture of an extracellular matrix in terms of microstructure and porosity. This scaffold allows for infiltration and proliferation of native cells and maintains sufficient space for native collagen deposition and blood vessel formation.3 The favorable outcome in this patient suggests that BBGFM is a promising adjunct in managing challenging wounds associated with coagulopathic sepsis and severe systemic illness. More broadly, our experience supports incorporation of bioactive glass technology into protocols for high-risk wounds in critical care settings.