(CS-078) Restoring Momentum in Stalled Wounds: A Three-Case Evaluation of Borate-Based Bioactive Glass Fiber Matrix (BBGFM) Therapy
Friday, April 10, 2026
Introduction: Chronic lower-extremity wounds including diabetic foot ulcers (DFUs) and venous leg ulcers (VLUs) pose significant clinical and economic burdens due to their prolonged healing trajectories and high recurrence rates.1 Impaired perfusion, bacterial burden, and chronic inflammation often inhibit progression through normal healing phases.2 Bioactive glass technologies have emerged as promising adjuncts because they provide a scaffold which allows for infiltration and proliferation of native cells while maintaining sufficient space for native collagen deposition and the formation of new blood vessels.3
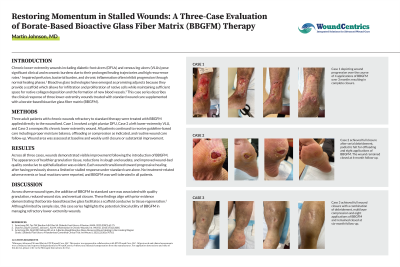
Methods: Six adult patients with chronic wounds refractory to standard therapy were treated with BBGFM applied directly to the wound bed. Case-1 involved a right plantar DFU, Case-2 a left lower-extremity VLU, and Case-3 a nonspecific chronic lower extremity wound. Case-4 involved a painful pretibial ulcer that was present for over two years and probed to bone with previous failed attempts to treat the wound with herbal medicine and refusal of debridement because of pain. Case - was a recurrent DFU that had not closed in over two years which had undergone 60 hyperbaric oxygen treatments at another facility. Case-6 was a recurrent painful VLU.
Results: Across the six cases, wounds demonstrated visible improvement following the introduction of BBGFM. The appearance of healthier granulation tissue, reductions in slough and exudate, and improved wound-bed quality conducive to epithelialization was evident. Each wound transitioned toward progressive healing after having previously shown a limited or stalled response. Specifically, Case-4 had four applications of BBGFM over 3-months resulting in complete closure. Case-5 achieved full closure after serial debridement, podiatric felt for offloading and eight applications of BBGFM. The wound remained closed at 6-month follow-up. Case-6 achieved full wound closure with a combination of debridement, multilayer compression and eight application of BBGFM and remained closed at six-month follow-up.
Discussion: Across diverse wound types, the addition of BBGFM to standard care was associated with quality granulation, reduced wound size, and eventual closure. These findings align with prior evidence demonstrating that borate-based bioactive glass facilitates a scaffold conducive to tissue regeneration.3 Although limited by sample size, this case series highlights the potential clinical utility of BBGFM in managing refractory lower-extremity wounds.

.jpg)