(CS-116) Multimodal Imaging for Point-of-Care Wound Assessment and Clinical Decision-Making
Friday, April 10, 2026
Adam Iddriss, MD; Star-Kayla Lewis, MD; Marisa Ranire-Maguire, MD; Amit Rao, MD
Introduction: Chronic wounds require etiology-specific assessment to guide timely interventions.1 Multimodal point-of-care imaging, including near-infrared spectroscopy (NIRS) for tissue oxygenation (StO2),2 thermography for skin surface temperature, and digital photography, offers non-invasive, real-time insights into perfusion, ischemia, and surrogate markers of infection.
Methods: A case series evaluated multimodal imaging in patients with lower extremity wounds. Assessments included overall perfusion via NIRS (StO2 levels), bilateral comparisons, periwound and wound bed analysis, and thermography for temperature gradients as surrogates for infection or inflammation.
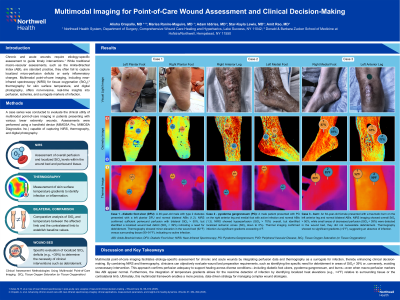
Results: Three cases illustrated etiology-based applications of multimodal imaging. Case 1: A 46-year-old male with type 2 diabetes presented with diabetic foot ulcer (DFU) on the left plantar foot (1.12 × 1.06 × 0.2 cm), no peripheral vascular disease (PVD), and normal ABI (1.2 bilaterally). NIRS revealed equivalent bilateral plantar StO2 (94-100%), confirming sufficient periwound perfusion, but localized wound bed StO2 of 0% indicated need for debridement. Thermography showed minor temperature elevation (92°F wound vs. 90-91°F surrounding), with no infection markers. Case 2: A male with pyoderma gangrenosum on the right anterior leg (7.43 × 4.7 × 0.1 cm) and infection; no PVD, normal ABI (1.32 left, 1.3 right). NIRS demonstrated StO2 >50% overall with localized hyperperfusion ( >70%), while thermography indicated infection via elevated wound temperature (89°F bed, 87°F periwound vs. 82-84°F leg). Case 3: A female with type 2 diabetes and a non-ischemic, non-infected right plantar DFU (1.92 × 1.75 × 0.3 cm); no PVD, ABI 0.99 left and 0.9 right (lower normal). NIRS confirmed StO2 >50% with localized 0% areas supporting debridement; thermography revealed cooler wound bed temperature (83°F vs. 89°F foot).
Discussion: Multimodal point-of-care imaging enables etiology-specific wound assessment by integrating perfusion data and using thermography as an infection surrogate. This approach helps identify debridement needs, evaluate perfusion adequacy, and detect inflammatory states, enhancing clinical decision-making and potentially improving patient outcomes across diverse wound etiologies.

.jpg)