
.jpg)
Case Series/Study
Buerger’s disease, (thromboangiitis obliterans), is a rare, non-atherosclerotic, segmental inflammatory vasculitis that primarily affects small- and medium-sized arteries and veins of the arms and legs impacting blood flow. The disease is typically found in the lower extremities, with skin ulceration and gangrene of the digits common, with pain being very intense1. The disease typically presents with distal extremity ischemia; common for the foot as an early site of involvement; often manifesting as digital ulceration, claudication, rest pain, or gangrene.
In the US, current estimations on prevalence are 12.6 – 20 cases per 100,000 population2.
Methods:
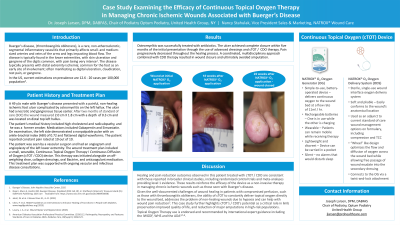
49 y/o male presented with Buerger’s disease and a non-healing painful ischemic foot ulcer with osteomyelitis on the left hallux with Necrotic and gangrenous tissue center. Size was 2.0CM X 1.8CM Depth 0.3CM on distal top left hallux after 2 months of SOC.
Patient history included high cholesterol, Radiculopathy, former smoker. Medications included Gabapentin and Simvastatin. Patient has non palpable pulse and ABI .72 on the left side with flattened digital wave forms. The patient had a Constant pain level of 10 / 10.
The patient was seen by a vascular surgeon and had an angiogram and angioplasty of the left lower extremity. The wound treatment plan included a small, wearable continuous topical oxygen / continuous diffusion of oxygen (cTOT / CDO) device, and was initiated alongside an off-weighting shoe, collagen dressings, oral Bactrim and anticoagulant medication. This was also supported with ongoing vascular and infectious disease consultations.
Results: Successful treatment of Osteomyelitis with antibiotics. Closure of the ulcer with dressings and CDO therapy in 5 months from patient presentation to the office and a reduction of pain throughout the healing process. The use of a multi team approach and the use of CDO therapy closed the wound and avoided amputation
Discussion:
Healing and pain reduction outcomes observed in this patient treated with cTOT / CDO, are consistent with those reported in broader clinical studies, including RCTs, and meta-analyses providing level 1 evidence. These results reinforce the efficacy of the device as a non-invasive therapy in managing chronic ischemic wounds such as those seen in Buerger’s disease.
Given the challenges of healing in patients with compromised perfusion, such as those with Thromboangiitis Obliterans, this case highlights the potential for cTOT to play a critical role in limb preservation, improved quality of life, and reduction of major amputations in high-risk populations.