
.jpg)
Clinical Research
Diabetic foot ulcers (DFUs) are a major contributor to lower-extremity amputations and wound-related morbidity in the United States. Infection and osteomyelitis are well-established clinical risk factors for poor healing outcomes. However, limited research has examined how microbial diversity and socioeconomic disparities jointly influence amputation risk. Understanding these relationships is essential for developing targeted interventions in high-risk populations.
We conducted a retrospective cohort study of 27,078 patients diagnosed with DFUs between 2019 and 2024 using data from the Indiana Network for Patient Care (INPC), a statewide health information exchange. Extracted variables included patient demographics, microbiological culture results, ICD/CPT codes for infection and amputation, and zip-code-level median household income. Logistic regression models were used to evaluate associations between infection type, presence of osteomyelitis, and likelihood of amputation. Geographic income data were used to assess socioeconomic patterns in DFU prevalence.
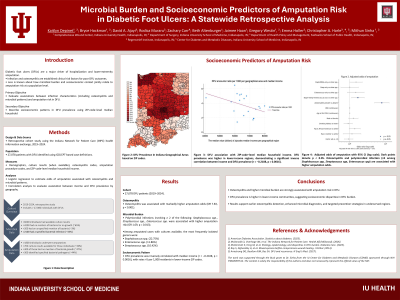
Osteomyelitis was associated with a 7.83-fold increase in odds of amputation (p < 0.001). Among amputated cases, the most frequently isolated pathogens were Staphylococcus spp. (22.75%), Enterococcus spp. (11.86%), and Streptococcus spp. (10.42%). Patients with polymicrobial infections involving all three genera had significantly elevated amputation risk (OR = 1.69, p = 0.013). DFU prevalence was inversely correlated with median income (r = -0.2108, p = 0.0016), with rates exceeding 5 per 1,000 residents in low-income zip codes.
This study demonstrates that microbial burden and osteomyelitis are strong predictors of amputation in DFU patients. Additionally, socioeconomic disparities relate to DFU prevalence and outcomes, suggesting that patients in underserved communities face additional risks. These findings support the need for enhanced microbial diagnostics, early osteomyelitis detection, and community-level wound care strategies. Public health should consider prioritizing resource allocation and preventive care in low-income regions to reduce amputation rates and improve healing trajectories. Of note, INPC aggregates data from across the state; however, variability in regional data contributions limits the accuracy of statewide estimates for DFU encounter frequency and the availability of bacteriology data.