(EBP-002) Pressure Injury Staging: Complementing Visual Assessment with Near-Infrared Spectroscopy and Thermography Imaging
Nirman Tulsyan, MD FACS RPVI – President, Heritage Wound Care
Introduction: Pressure injuries (PIs) represent a global healthcare challenge.1 Accurate staging of PIs is critical for effective management, yet reliance on subjective visual assessment has been associated with misstaging rates of up to 69%.2 This case series compares traditional visual assessment with near-infrared spectroscopy (NIRS) and infrared thermography imaging to complement and enhance staging accuracy by detecting subsurface physiological changes. While previous studies have shown that NIRS and thermography can aid in early pressure injury detection,3 this study investigates their potential to improve PI staging accuracy.4,5
Methods: A case series was conducted, including 2 representative patients for each PI stage (Stages 1–4). Each case underwent retrospective visual inspection using point-of-care digital images, NIRS to assess tissue oxygenation and perfusion, and thermography to evaluate temperature variations related to perfusion and/or inflammation. The study aimed to compare how each modality characterizes tissue changes across PI stages.
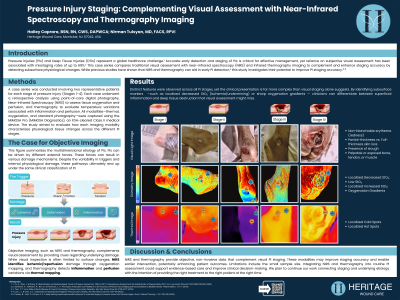
Results: Distinct features were observed across modalities for each stage. Stage 1: Intact skin with erythema; NIRS showed reduced StO₂ (79% vs 83% in healthy skin, , with an increase to >90% at the center), and thermography detected a small cold spot (~2.7°F). Stage 2: Partial-thickness skin loss; NIRS showed decreased oxygenation in surrounding tissue (65%) with higher StO₂ in the wound bed (81% vs 70% healthy skin), while thermography revealed persistent periwound cold spots. Stage 3: Full-thickness skin loss; NIRS indicated perfusion deficits in periwound tissue (67%) and very low oxygenation in slough (~39%, locally 0%), with thermography showing broader temperature gradients. Stage 4: Full-thickness tissue loss with exposed structures; NIRS revealed highest StO₂ in subcutaneous tissue (84%), followed by healthy skin (75%), and periwound tissue (64%), with thermography reflecting deeper tissue involvement through pronounced cold and hot zones.
Discussion: NIRS and thermography provide objective, noninvasive data that complement visual PI staging. These modalities may improve staging accuracy and enable earlier intervention, potentially enhancing patient outcomes. Limitations include the small sample size and inclusion of only one case per stage. Integrating NIRS and thermography into routine PI assessment could support evidence-based care and improve clinical decision-making.

.jpg)