
.jpg)
Case Series/Study
Lymphatic leaks represent significant complications following vascular surgery, contributing to delayed wound healing and increased patient morbidity and infection rates. Management includes conservative measures and operative techniques, such as lymphatic ligation and muscle flaps.1,2 Muscle flaps are frequently employed for obliterating dead space and demonstrate high success rates, reported at approximately 95%.3
Methods:
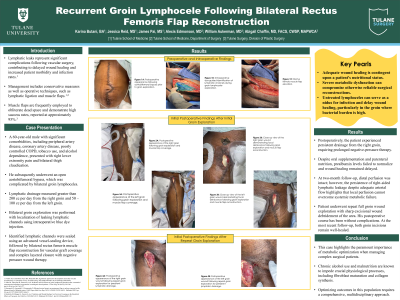
A 60-year-old male with significant comorbidities, including peripheral artery disease, coronary artery disease, poorly controlled COPD, tobacco use, and alcohol dependence, presented with right lower extremity pain and bilateral thigh claudication. He subsequently underwent an open aortobifemoral bypass, which was complicated by bilateral groin lymphoceles. His treatment course involved bilateral muscle flap reconstruction, intraoperative lymphatic channel localization using blue dye, LigaSure sealing, and negative pressure wound therapy.
Results:
Postoperatively, the patient experienced persistent drainage from the right groin wound, requiring prolonged negative-pressure therapy. Despite oral supplementation and a course of intravenous total parenteral nutrition, objective markers of malnutrition failed to normalize, and wound healing remained delayed. At two-month follow-up, distal perfusion was intact; however, ongoing right-sided lymphatic leakage and poor nutritional recovery continued to impede full resolution. During this evaluation, he was found to have a delayed, recurrent right-sided lymphocele that required operative exploration; the rectus femoris flap was viable and intact, the anastomosis remained well-covered, and the superficial wound tract was excised. Following this procedure, the wound gradually granulated and ultimately healed with continued negative-pressure therapy and improved nutritional support.
Discussion:
This case highlights the paramount importance of metabolic optimization when managing complex surgical patients. Adequate wound healing is contingent upon a patient's nutritional status. Chronic alcohol use and malnutrition are known to impede crucial physiological processes, including fibroblast maturation and collagen synthesis.4 This case illustrates that severe, persistent metabolic dysfunction can result in the failure of otherwise reliable surgical reconstructions. Optimizing patient outcomes in this population necessitates a comprehensive, multidisciplinary approach to management.