(CS-154) Clinical Outcomes of Cold Atmospheric Plasma Therapy for Chronic Diabetic Foot Ulcers, Venous Leg Ulcers, and Pressure Ulcers
Friday, April 10, 2026
Leandro Garcia, MD – SerenaGroup, Inc.; Meghan Neil, NP-C – SerenaGroup, Inc.; Laura Serena, LPN, RN, MS – Chief Research Officer, SerenaGroup, Inc.; Michaela Wadsworth, MPAS, PA-C – SerenaGroup, Inc.; Colleen O’Malley, MS – SerenaGroup, Inc.
Introduction: Chronic wounds such as diabetic foot ulcers (DFUs), venous leg ulcers (VLUs), and pressure ulcers are slow to resolve and impose significant clinical and economic burdens. Their prolonged course is frequently driven by impaired perfusion, chronic inflammation, microbial load, and patient comorbidities, which collectively limit responsiveness to standard care. Cold atmospheric plasma (CAP) has emerged as an adjunctive modality capable of generating reactive oxygen and nitrogen species that exert broad-spectrum antimicrobial activity while stimulating pathways involved in cellular repair, angiogenesis, and immune modulation. This study evaluated the early therapeutic effect and safety profile of CAP in individuals with long-standing, treatment-resistant ulcers.
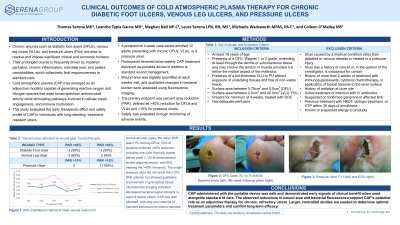
Methods: A prospective 4-week case series enrolled 12 adults presenting with chronic DFUs, VLUs, or a pressure ulcer. Participants received twice-weekly CAP treatment delivered via portable device in addition to standard wound management. Wound area was digitally quantified at each weekly visit, and qualitative changes in bacterial burden were assessed using fluorescence imaging. The primary endpoint was percent area reduction (PAR), defined as >40% reduction for DFUs and VLUs and >10% for pressure ulcers. Safety was evaluated through monitoring of adverse events.
Results: Across all ulcer types, the mean PAR was 21%. Among DFUs, 50% of subjects achieved >40% reduction, including one ulcer that fully closed before week 4. VLUs demonstrated similar responsiveness, with 60% meeting the >40% threshold. The single pressure ulcer did not reach the ≥10% PAR criterion but showed qualitative improvement in granulation tissue. Fluorescence imaging indicated decreased bacterial signal intensity in eight of twelve ulcers. CAP was well tolerated, with only one instance of transient periwound erythema reported.
Discussion: CAP administered with the portable device was safe and demonstrated early signals of clinical benefit when used alongside standard of care. The observed reductions in wound area and bacterial fluorescence support CAP’s potential role as an adjunctive therapy for chronic, refractory ulcers. Larger, controlled studies are needed to determine optimal treatment parameters and confirm long-term efficacy.

.jpg)