
.jpg)
Health Economics
Skin substitutes offer long-established clinical benefit for diabetic foot ulcers (DFUs), yet their comparative cost-effectiveness remains under-characterized. The purpose of this study was to evaluate the cost-effectiveness of ten skin substitutes for DFU management in a hospital outpatient department (HOPD) setting, based on healing outcomes and treatment costs.
Methods:
This study utilizes published clinical data combined with Centers for Medicare and Medicaid Services (CMS) Q3 2025 HOPD and Physician Fee Schedule (PFS) facility rates to compare 10 skin substitutes (denoted A-J) used for treating DFUs in HOPD settings. Healing rates were compared, and cost-effectiveness was analyzed.
Results:
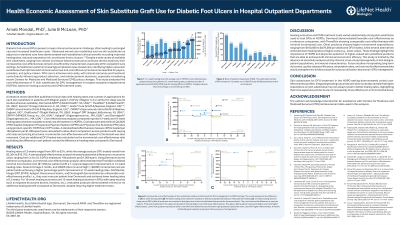
Considerable variation was observed in both costs and healing rates among skin substitutes used for DFUs in HOPD. Healing rates at 12 weeks ranged from 30% to 62%, while the average cost per DFU treated varied from $2,304 to $16,702. Cost-effectiveness analysis revealed substantial differences across products, with the number of DFUs healed per 100 patients per $1,000 spent ranging from 3.4 to 23.0. Using an acellular dermal matrix (ADM; A)1 as the reference comparator, incremental cost-effectiveness analysis showed that split-thickness living skin graft (B)2 had minimal cost difference and a slightly higher healing rate. A fish skin graft(C)3, a placental membrane product(D)4, and a tri-layer wound matrix(E)5 demonstrated substantially higher incremental costs with slight increase in healing compared to ADM. Several other products including an additional acellular human dermal matrix(F)1, a bioengineered bilayer dermal regeneration template(G)6, a dehydrated amnion/chorion membrane amniotic membrane allograft(H)7, a bioengineered living skin substitute(I)7, and a human fibroblast-derived product(J)8 had lower 12-week healing rates despite incurring similar or greater costs. For a 16-week healing timeframe and DFUs with exposed structures, all products provided limited additional healing relative to costs when compared to the reference.
Discussion:
Skin substitutes for DFU treatment in the HOPD setting demonstrated varied cost-effectiveness profiles. Integrating healing outcomes with direct cost data reveals that higher cost for skin substitutes may not always result in better healing rates, highlighting that more expensive products are not necessarily more effective.