(CS-122) Protocol Implementation and Case Series for Reconstruction of Stage 4 Ulcers with Osteomyelitis
Friday, April 10, 2026
Jitendra Singh, MD; Chiagozie Nwakanma, MD; Scott Gorenstein, MD
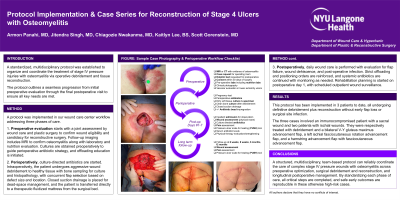
Introduction: A standardized, multidisciplinary protocol was established to organize and coordinate the treatment of stage IV pressure injuries with osteomyelitis via operative debridement and tissue reconstruction. The protocol outlines a seamless progression from initial preoperative evaluation through the final postoperative visit to ensure all key needs are met.
Methods: A protocol was implemented in our wound care center workflow addressing three phases of care: preoperative, perioperative, and postoperative. Preoperative evaluation starts with a joint assessment by wound care surgery and plastic surgery to confirm wound eligibility and candidacy for reconstructive surgery. Follow-up imaging includes MRI to confirm osteomyelitis along with laboratory and nutrition evaluation. Cultures are obtained preoperatively to guide perioperative antibiotic strategy, and offloading education is initiated. Perioperatively, culture-directed antibiotics are started. Intraoperatively, the patient undergoes aggressive wound debridement to healthy tissue with bone sampling for culture and histopathology, with concurrent flap selection based on defect size and location. Closed suction drainage is placed for dead-space management, and the patient is transferred directly to a therapeutic fluidized mattress from the surgical bed. Postoperatively, daily wound care is performed with evaluation for flap failure, wound dehiscence, and post-operative infection. Strict offloading and positioning orders are reinforced, and systemic antibiotics are continued with monitoring as needed. Rehabilitation planning is started on postoperative day 1, with scheduled outpatient wound surveillance.
Results: The protocol has been implemented in 3 patients to date, all undergoing definitive debridement plus reconstruction without early flap loss or surgical site infection. The three cases involved an immunocompromised patient with a sacral wound and two patients with ischial wounds. Following MRI-confirmation of osteomyelitis, they were respectively treated with debridement and a bilateral V-Y gluteus maximus advancement flap, a left ischial fasciocutaneous rotation advancement flap, and a hamstring advancement flap with fasciocutaneous advancement flap.
Discussion: A structured, multidisciplinary, team-based protocol can reliably coordinate the care of complex stage IV pressure wounds with osteomyelitis across preoperative optimization, surgical debridement and reconstruction, and longitudinal postoperative management. By standardizing each phase of care, all critical steps are completed and safe early outcomes are reproducible in these otherwise high-risk cases.

.jpg)