
.jpg)
Case Series/Study
Chronic neuropathic foot ulcers attributed to diabetes, charcot neuroarthopathy, and peripheral neuropathy can cause loss of protective sensation, foot deformities, and autonomic skin changes.
Impaired healing and frequent bacterial colonization with biofilm make management difficult. Standard of care can include offloading, debridement, revascularization, infection control, and physiologic dressings. Advanced therapies are recommended for wounds failing to improve by 50% after four weeks.
Decellularized dermal matrix is an effective adjunct for unresponsive ulcers, providing a scaffold for cell infiltration and tissue regeneration. Recent RCTs show improved healing rates and faster closure.
Methods:
A 66-year-old morbidly obese, male patient presented with a chronic neuropathic ulcer on the plantar aspect of the left foot, persisting for more than five years, reflecting significant underlying sensory neuropathy, structural foot deformity, and a persistently impaired healing environment. Failed treatments included various skin substitutes and biologic dressings.
A comprehensive, multimodal strategy was initiated including a series of applications of decellularized dermal matrix, selected to provide a scaffold that supports cellular infiltration, angiogenesis, and tissue regeneration. Additionally, total contact casting achieved consistent offloading of plantar pressures, in addition to targeted lymphedema therapy to reduce chronic swelling, improve microcirculation, and enhance delivery of oxygen and nutrients. The combined approach aimed to correct the mechanical, biologic, and inflammatory barriers to healing and to optimize conditions for successful wound closure.
Results:
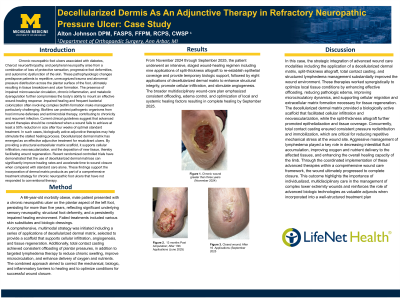
From November 2024 through September 2025, the patient underwent an intensive, staged wound-healing regimen including nine applications of split-thickness allograft to re-establish epithelial coverage and provide temporary biologic support, followed by eight applications of decellularized dermal matrix to enhance structural integrity, promote cellular infiltration, and stimulate angiogenesis.
The broader multidisciplinary wound-care plan emphasized consistent offloading, edema control, and optimization of local and systemic healing factors resulting in complete healing by September 2025.
Discussion:
This complex case highlights the need for multimodal care when standard therapies fail. Strategic use of decellularized dermal matrix, of split-thickness allograft, total contact casting and lymphedema management, improved the wound environment by enhancing offloading, reducing edema, and supporting cellular regeneration, leading to complete healing and underscoring the value of advanced biologics within a comprehensive treatment strategy.