(CS-024) Using a Biomimetic Matrix in Treatment-Resistant Wounds with Autoimmune Etiologies
Friday, April 10, 2026
Garismar Ramirez, BS; John Lantis, MD
Introduction: Chronic wounds driven by autoimmune conditions such as rheumatoid arthritis and pyoderma gangrenosum are characteristically refractory to standard wound care modalities due to persistent inflammation, impaired extracellular matrix (ECM) remodeling, and heightened susceptibility to infection. These patients often experience prolonged healing trajectories and multiple treatment failures. A Biomimetic Matrix* engineered to emulate the architecture of native human ECM, while also forming a protective antibacterial barrier is an approach to healing these types of wounds. By offering a non-immunogenic 3D matrix, this product may facilitate cellular migration, granulation, and progressive wound closure in environments where conventional therapies are insufficient. This study aimed to evaluate whether weekly application of the Biomimetic Matrix* could accelerate healing in two chronic, treatment-resistant wounds of autoimmune etiology.
Methods: Biomimetic Matrix* was applied once weekly to two refractory lower extremity wounds, one caused by rheumatoid arthritis and the other by pyoderma gangrenosum. Patients underwent wound debridement and irrigation in a vascular office setting, followed by application of the matrix using the pre-filled syringe. Wounds were covered with a non-adherent dressing, and weekly assessments were performed for up to six weeks, including wound measurements and qualitative tissue assessment.
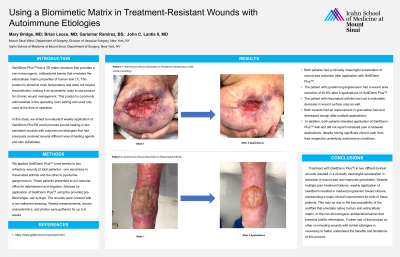
Results: Both patients demonstrated a clinically meaningful acceleration in wound healing. The pyoderma gangrenosum wound achieved a 40.8% reduction in area after five weekly applications. The rheumatoid arthritis associated wound also showed a marked decrease in surface area and improvement in granulation tissue. In both cases, slough burden diminished visibly over the treatment period. The product was well tolerated, and neither patient experienced increased pain between applications despite significant baseline chronic pain.
Discussion: Treatment with a Biomimetic Matrix* in two difficult-to-treat wounds resulted in wound area reduction and improved granulation. Despite multiple prior treatment failures, weekly application of this product resulted in progression toward closure, representing a major clinical improvement for both patients. This may be due to the biocompatibility of the ECM that emulates native human skin, or the non-immunogenic antibacterial barrier that prevents biofilm reformation. Further use of this product on other non-healing wounds with similar etiologies is necessary to better understand the benefits and limitations of this product.

.jpg)