
.jpg)
Case Series/Study
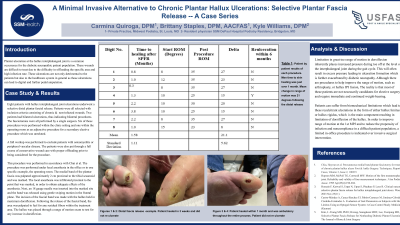
Plantar ulceration at the hallux interphalangeal joint is a common occurrence for the diabetic neuropathic patient population. These wounds are difficult to treat due to the difficulty in offloading the specific area and high infection rate. These ulcerations are not only detrimental to the patients but also to the healthcare system in general as these ulcerations can lead to digital and further pedal amputation. The procedure was performed under local anesthesia in the office or in one specific example, the operating room. The medial band of the plantar fascia was palpated approximately 2 cm proximal to the tibial sesamoid and was marked. The local anesthesia was infiltrated proximal to the point that was marked, in order to obtain adequate effects of the anesthesia. Next, an 18 gauge needle was inserted into the marked site and the band was released using gentle swiping motion in the frontal plane. The incision of the fascial band was made with the hallux held in maximum dorsiflexion. Following the release of the fascial band, the area was palpated to feel for any residual fibers within the treatment area. The hallux was placed through a range of motion exam to test for any increase in dorsiflexion. In each of the seven patients within the case series, healing of the wound was achieved following the limited fasciotomy. The average amount of dorsiflexion of the MTPJ increased by an average of 21 degrees. The ranges of dorsiflexion began at only 8 degrees with end dorsiflexion being 35 degrees. Although this is a limited sample size, with a 100% rate of healing, it is difficult to deny the procedures success. Procedure was statistically significant at a p-value of 0.00006. Standard deviation of 5.62 was calculated. Limitation in great range of motion dorsiflexion inherently places increased pressure during toe off at the level of the interphalangeal joint during the gait cycle. This will often result in excess pressure leading to ulceration formation which is further exacerbated by diabetic neuropathy. Patients can suffer from biomechanical limitations which lead to these recalcitrant ulcerations in the form of either hallux limitus or hallux rigidus, which is the main component resulting in limitation of dorsiflexion of the hallux. In order to improve range of motion at the 1st MPJ and to reduce the propensity of infection and noncompliance in a difficult patient population, a limited in-office procedure is indicated over invasive surgical intervention.
Methods:
Results:
Discussion: