(CR-055) Interim analysis of cellular, acellular, and matrix-like products for the management of chronic lower extremity ulcers in the STABLECAMP trial
Friday, April 10, 2026
Brianna Tramelli, BS – SerenaGroup, Inc.; Emily King, MS – SerenaGroup, Inc.; Dereck Shi, MS – SerenaGroup, Inc.; Madison Dunn, MS – SerenaGroup, Inc.; Manisha Mehta, DPM – GFC of Southeastern Michigan; R Pavelescu, DPM, FACFAS, FRCPS(Glas) – The Foot, Ankle, & Vein Specialists; David Simon, DPM FACFAS – Mount Sinai Brooklyn Hospital
Introduction: Chronic lower extremity ulcers, including diabetic foot ulcers (DFUs) and venous leg ulcers (VLUs), remain difficult to heal, contributing to substantial patient morbidity and economic burden. Standard of care (SOC) often results in delayed or incomplete wound closure. Cellular, acellular, and matrix-like products (CAMPs) have emerged as therapies intended to accelerate wound closure.
Methods: An interim analysis of the STABLECAMP trial examined how several CAMPs + SOC perform in comparison with SOC alone. The primary endpoint was percentage of ulcers achieving complete wound closure in 12 weeks, defined as 100% re-epithelialization without drainage for two consecutive weeks.
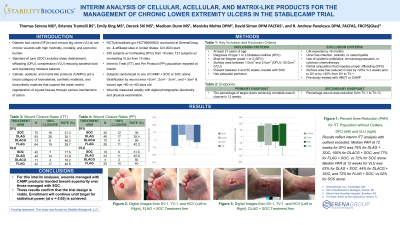
Results: Baseline characteristics were balanced across treatment groups at the time of interim analysis. In the DFU cohort, the dual layer amnion/chorion membrane allograft (DLACG) with SOC arm achieved a 58.3% closure rate in the Intent-To-Treat (ITT) analysis compared with 13.3% for SOC alone, a statistically significant 45% absolute gain (n = 12, 95% CI 15.7% to 68.4%, p = 0.001, α = 0.05). In Per Protocol (PP), the four layer amniotic membrane allograft (FLAG) with SOC arm achieved 63.6% closure versus 23.8% with SOC alone, also reaching statistical significance at a 39.8% absolute gain (n = 11, 95% CI 4.5% to 64.8%, p = 0.027, α = 0.05). No other DFU treatment groups showed statistical significance. Across both ITT and PP analyses, all CAMP arms had greater mean and median percent area reduction (PAR) than SOC. For VLUs, dual layer, amniotic membrane allograft (DLAG) + SOC yielded a 50% closure rate in ITT compared with 16.7% for SOC alone, representing a statistically significant 33.3% absolute gain (n = 20, 95% CI 5.6% to 55.8%, p = 0.018, α = 0.05). No other treatment groups were significant in ITT or PP. PAR outcomes favored DLAG + SOC for both ITT and PP.
Discussion: The interim results indicate that CAMPs + SOC may enhance wound closure outcomes for both wound types compared with SOC alone. Significant improvements were observed for DLACG in DFUs and DLAG in VLUs within ITT analyses. These preliminary findings support continued investigation of CAMPs as a potential regenerative option for chronic wound management.

.jpg)