(CS-114) Coordination of team-based protocol for advanced pelvic pressure injury surgery for optimal success: a case series
Friday, April 10, 2026
Ireland Coates, MS – Lakeview Hospital; Oygul Mirzalieva, PhD – LSU Health Sciences Center School of Medicine; Kaylie Miceli, NP – Tulane School of Medicine; James Pai, MS – Tulane School of Medicine; Jessica Reid, MS – Tulane School of Medicine; John Holtrop, MD – Department of Surgery, Division of Plastics and Reconstructive Surgery – Tulane School of Medicine; Abigail Chaffin, MD, FACS, CWSP, MAPWCA – Department of Surgery, Division of Plastics and Reconstructive Surgery – Tulane School of Medicine
Introduction: While several plastic surgery operations are available for the treatment of ischial and sacral pressure injuries (PIs), flap failure rates remain 65–80%.1 Complications including incision dehiscence, infection, and recurrent breakdown most often reflect lapses in perioperative care, particularly inadequate offloading during transfers and inconsistent use of pressure-redistributing surfaces.1,2 This report describes the implementation of a multidisciplinary PI protocol at a community hospital designed to improve flap outcomes and support surgeon participation.
Methods: The protocol requires involvement from plastic surgery, wound care nurse practitioners, hospital medicine, infectious disease, vascular and orthopedic surgery, and dermatology. Preoperatively, comorbidities are optimized through glycemic control in diabetic patients, stabilization of cardiovascular disease, and complete nicotine cessation. Nutritional assessment includes measurement of albumin, prealbumin, zinc, and vitamins A, C, and E, with targeted supplementation. A comprehensive infection evaluation is performed, with wound care and debridement when indicated.3
Postoperatively, patients are transferred using appropriate offloading technique to the long-term acute care hospital (LTACH), where they receive pressure redistribution on an air-fluidized sand bed, incisional negative pressure wound therapy, and follow a staged sitting protocol. Infrared thermography may be used as an adjunct for early detection of flap compromise.3
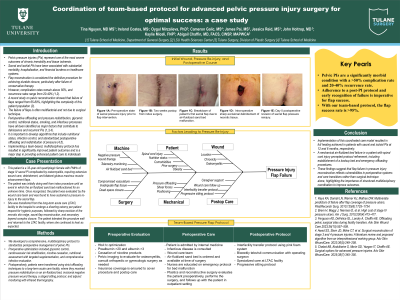
Results: Several cases demonstrate the protocol’s effectiveness. A 67-year-old man with a sacral pressure injury and stage 3 kidney disease achieved full flap healing after one year in the outpatient wound center. A 43-year-old woman with a 25-year history of T7 paraplegia achieved complete healing of a chronic stage 4 right ischial injury after six months. A 33-year-old woman with C2–C4 spinal cord injury, initially a surgical success, subsequently developed a 6 × 3 cm area of necrosis after an LTACH air-fluidized bed malfunction; rapid multidisciplinary communication enabled flap salvage.
Discussion: Implementation of the proposed multidisciplinary protocol within a coordinated system of care resulted in a 95% flap success rate. The mechanical failure prompted protocol refinement, including maintaining a backup air-fluidized bed and establishing emergency offloading procedures.3 Such vigilance is essential to prevent flap compromise, infection, and systemic morbidity.

.jpg)