
.jpg)
Case Series/Study
Three patients with multiple serious comorbidities (including cerebral vascular accident, coronary artery disease, deep venous thrombosis, Charcot deformity, history of amputation, infection / gangrene) presenting with complex, hard-to-heal diabetic foot ulcers (4 wounds total), at risk for below-the-knee amputation, were selected to receive BMM. All wounds were extensive and full-thickness, involving exposed structures (Wagner 2-4). Wounds were extensively debrided to remove devitalized tissue (including biofilm, exudate, necrotic tissue, fibrin, and slough) prior to BMM application following the manufacturer’s instructions. Wound characteristics were assessed at baseline and during follow-up visits.
Results:
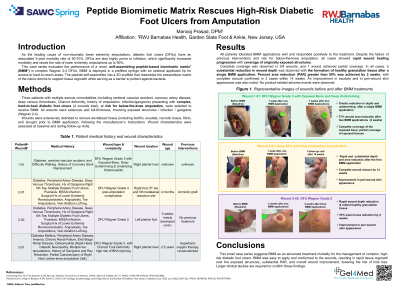
All patients tolerated BMM applications well and responded positively to the treatment. Despite the failure of previous interventions and risk for below-the-knee amputation, all cases showed rapid wound healing progression resulting in complete (3/4) or partial (1/4) coverage of the originally exposed structures. In all cases, a substantial reduction in wound depth was observed with the formation of healthy granulation tissue after a single application. Percent area reduction (PAR) greater than 50% was achieved by 2 weeks, with complete closure confirmed in 2 cases within 14 weeks. An improvement in exudate and in peri-wound skin appearance was also noted. No product-related adverse events were observed.
Discussion:
This case series suggests BMM as an advanced treatment modality for the management of complex, high-risk diabetic foot ulcers. BMM was easy to apply and conformed to the wounds, resulting in rapid tissue regrowth over the exposed structures, substantial PAR, and overall wound improvement, lowering the risk of limb loss. Larger clinical studies are required to confirm these findings.