(CS-030) Defying Pathergy: Excisional Sharp Debridement and Skin Grafting in Advanced Pyoderma Gangrenosum
Abigail Chaffin, MD, FACS, CWSP, MAPWCA; Eva Murphy, BS; James Pai, MS; Jessica Reid, MS
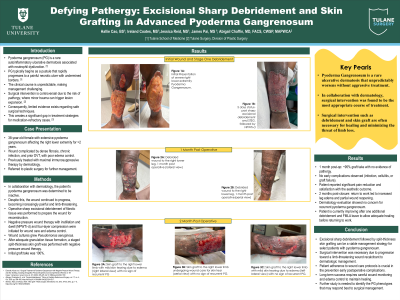
Introduction: Pyoderma gangrenosum (PG) is a rare autoinflammatory ulcerative dermatosis driven by neutrophil dysfunction. It typically begins as a pustule that rapidly progresses to a painful, necrotic ulcer with undermined borders. Surgical intervention in PG is controversial due to the risk of pathergy, an exaggerated inflammatory response to trauma that can worsen disease severity. Consequently, limited guidance exists regarding operative management in medication-refractory or limb-threatening cases. We report a case demonstrating successful surgical reconstruction in advanced PG using a multidisciplinary approach.
Methods: A 38-year-old woman with extensive PG of the right lower extremity was referred after failing maximal immunosuppressive therapy and experiencing progressive ulcer expansion. Her course was complicated by dense fibrosis, chronic wound colonization, massive edema in the setting of prior deep venous thrombosis, and failure of conservative wound care. Given the limb-threatening nature of the wound, dermatology and plastic surgery jointly determined that surgical intervention was warranted despite the theoretical risk of pathergy. The patient underwent aggressive sharp excisional debridement to viable subcutaneous adipose tissue to remove inflamed and nonviable tissue. Post-debridement, irrigating negative-pressure wound therapy was applied to reduce bioburden and promote granulation. An extracellular matrix scaffold was then placed to optimize the wound bed, followed by immediate split-thickness skin grafting to achieve definitive closure and re-epithelialization. Postoperative care emphasized edema control and close dermatologic surveillance.
Results: At one month postoperatively, approximately 95% graft take was observed with no evidence of infection, cellulitis, or graft loss. The patient reported significant pain reduction and satisfaction with the aesthetic outcome. Follow-up demonstrated durable wound closure and stable edema. No pathergic reaction occurred at the graft site, though a limited donor-site reaction was monitored without complication. No disease recurrence has been observed to date.
Discussion: This case illustrates that excisional sharp debridement with immediate split-thickness skin grafting can be a viable option for select patients with severe, refractory PG. Careful patient selection, meticulous surgical technique, aggressive postoperative management, and close multidisciplinary coordination are critical to minimizing pathergy risk and achieving favorable outcomes. Further studies are needed to identify PG phenotypes most likely to benefit from surgical intervention.

.jpg)