(CS-101) Novel Use of Microfluid Jet Therapy for Wound Bed Preparation in Venous Ulcers and Facilitated Extraction of Calcinosis Cutis
Friday, April 10, 2026
William Tsiaras, MD, PhD – Clinical Director, Dermatology, Angiogenesis & Wound Healing Center, Mass General Brigham, Harvard Medical School; Noemi Li, student; William Li, MD – President and CEO, Angiogenesis Foundation
Introduction: Chronic venous leg ulcers can be complicated by lipodermatosclerosis and dystrophic calcinosis cutis, which pose major challenges to wound bed preparation, infection control, and pain management. Calcinosis cutis results in hard, adherent calcium deposits that impede healing and make traditional debridement difficult and painful. Microfluid jet therapy is an emerging advanced wound therapy that applies a precision, high-pressure fluid stream for selective removal of slough, biofilm, and necrotic tissue and induces microbleeding to stimulate angiogenesis and granulation tissue. Its application for loosening calcific deposits has not previously been described.
Methods: We report using microfluid jet therapy in a 79-year-old female with an 18-month nonhealing right pretibial ulcer associated with chronic venous stasis, lipodermatosclerosis, and calcinosis cutis. Radiography revealed extensive subcutaneous calcifications beneath the wound. She had a history of recurrent soft-tissue infections, failed split-thickness skin grafts, and unsuccessful medical therapy with doxycycline and colchicine. Regular outpatient debridement with surgical extraction of calcium deposits required opioid analgesia for procedural pain. As an alternative, microfluid jet therapy* using hypochlorous solution was initiated for wound-bed preparation.
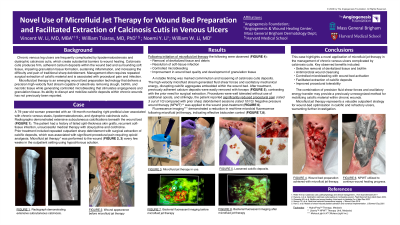
Results: Following initiation of microfluid jet therapy, the wound demonstrated effective removal of devitalized tissue, resolution of soft-tissue infection, and improved wound bed quality characterized by controlled microbleeding and subsequent fibrovascular tissue. A key observation was the marked comminution and loosening of calcinosis cutis deposits. The high-velocity microfluid stream generated fluid shear forces and oscillatory energy that disrupted and weakened the calcific aggregates. Once treated, these deposits were easily removed using forceps, in contrast to the prior requirement for surgical extraction. The patient also reported substantially reduced procedural pain.
Discussion: This case illustrates that microfluid jet therapy is a promising treatment innovation for complex venous ulcers complicated by calcinosis cutis. The combination of selective debridement, antimicrobial cleansing, controlled microbleeding with wound bed activation, and microfluid jet-generated shear and oscillatory forces that disrupt calcific deposits represents a novel, well-tolerated approach to wound-bed optimization and calcinosis cutis. These findings support further investigation into the mechanism and broader applicability of microfluid jet therapy in calcific and refractory wound pathology.

.jpg)