(CR-042) Association of Bacterial Fluorescence with Early Response to Skin Substitutes in Diabetic and Venous Ulcers: A Single-Blinded Prospective Study
Friday, April 10, 2026
Amit Rao, MD – Senior Clinical Research Coordinator, Comprehensive Wound Healing & Hyperbaric Center, Northwell Health; Sally Kaplan, RN, CCRC – Research Nurse Specialist, Comprehensive Wound Healing & Hyperbaric Center, Northwell Health; Farisha Baksh, BS – Clinical research coordinator, Comprehensive Wound Healing & Hyperbaric Center, Northwell Health; Julie Isgro, MSN, ANP-C, CWOCN – Nurse Practitioner, Comprehensive Wound Healing Center & Hyperbaric Oxygen, Northwell Health; Adam Iddriss, MD; Christina Del Pin, MD, FACS
Introduction: Chronic wounds can require skin substitutes, or Cellular, Acellular, or Matrix-type products (CAMPs), when standard therapies fail to achieve healing [1]. Although CAMPs can expedite wound closure and promote tissue regeneration, infection and elevated bacterial burden may reduce their effectiveness by degrading the matrix and consuming oxygen and nutrients [2-4]. Bacterial fluorescence imaging (BFI) using a handheld device* enables bedside, real-time visualization of elevated bacterial loads (≥10⁴ CFU/g) [5-7]. Because significant bacterial burden often remains undetected on clinical examination [8-10], detecting it before CAMP application is important. This study evaluated whether the presence or absence of bacterial fluorescence immediately before CAMP placement was associated with early wound area reduction as a therapeutic response in chronic ulcers.
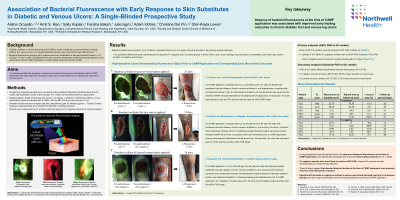
Methods: This single-blinded, prospective observational study enrolled patients (N=10) at a wound center with uninfected diabetic and venous ulcers indicated for CAMP treatment. Each wound underwent standard wound bed preparation, including cleansing and debridement, followed by BFI evaluation immediately before CAMP application. Wounds were categorized as positive or negative with the presence or absence of red or cyan fluorescence signals detected by the device*, indicating elevated bacterial burden. Healing response was evaluated by percentage area reduction (PAR) at 4±1 weeks post-applicationusing digital wound measurements. Primary endpoint was wound healing of 40% percentage area reduction (PAR).
Results: Eighty percent of nonfluorescent wounds achieved at least 40% of PAR. None of the fluorescent wounds healed as fast (p< 0.05). Mean wound area change differed significantly between groups; fluorescence-negative wounds showed a 68% mean reduction in area compared with a 34% mean increase among fluorescence-positive wounds (p< 0.05).
Discussion: This pilot study found a significant association between the presence or absence of bacterial fluorescence in the wound at the time of CAMP application and early healing outcomes. Fluorescence-negative wounds were more likely to achieve positive healing, whereas fluorescence-positive wounds showed poor outcome. Fluorescence imaging can help clinicians confirm wound bed bacterial load before advanced therapy. Integrating fluorescence-guided assessment into clinical practice may standardize wound evaluation and optimize CAMP application in chronic wound care.

.jpg)