(CS-133) Multimodal Thermal and Fluorescence Imaging in Advanced Wound Care: A Case Series Using an All-in-One Wound Imaging Device
Friday, April 10, 2026
Ron Linden, BSc, MD, CCF, DRCPSC, MSM – Medical Director, Judy Dan Centre for Hyperbaric Medicine & Advanced Wound Care, Judy Dan Research and Treatment Centre, North York, Ontario, Canada; Laura Jones-Donaldson, PhD – Director of Clinical Trials & Education, MolecuLight Inc.; Danielle Dunham, MHSc – Director of Marketing and Product Management, MolecuLight Inc.
Introduction: Conventional wound assessment methods offer limited insight into wound physiology, but advances in digital imaging now enable more comprehensive wound evaluations and improved patient care. Fluorescence imaging is a validated point-of-care technique for detecting clinically significant bacterial burden (≥10⁴ CFU/g) in real time [1-3]. Thermal imaging provides a contact-free, non-invasive method to assess tissue perfusion, and inflammation or infection through analysis of skin-surface temperature gradients [4, 5]. By translating infrared radiation into temperature maps, thermography reveals physiological changes associated with infection or healing [6, 7]. The integration of fluorescence and thermal imaging represents an important, multimodal approach to wound assessment. This case series demonstrates the clinical use of multimodal thermal and fluorescence imaging in chronic wound assessment.
Methods: This descriptive case series evaluated patients with chronic wounds of mixed etiologies using a handheld class II medical device* capable of capturing co-registered standard, thermal infrared, and bacterial fluorescence images. Thermal imaging was used to assess temperature differences between the wound, periwound, and contralateral limb, while fluorescence imaging was used to detect bacterial burden in the wound or periwound.
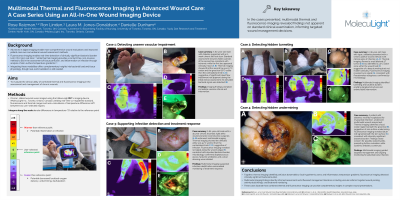
Results: Thermal imaging revealed localized perfusion impairment, and inflammation not visible on standard clinical inspection, while fluorescence imaging identified elevated bacterial signals indicative of clinically significant bacterial burden. Areas showing lower temperatures relative to surrounding tissue indicated perfusion compromise or regions with undermining or tunneling, confirmed by probing, prompting vascular referral and early intervention in one instance. In contrast, increased temperature zones aligned with inflammation and infection, with fluorescence signals highlighting bacterial burden within the wound bed or periwound area, confirmed by microbiological analysis.
Discussion: This case series highlighted the practical, real-world use of multimodal imaging device* in wound management. Integrating thermal and fluorescence imaging demonstrated strong potential as a complementary, objective approach for assessing chronic wounds. By concurrently visualizing temperature variations and bacterial burden, multimodal imaging provided critical insights into the underlying wound environment at point-of-care, enabling earlier recognition of potential wound complications and supporting healing through timely, targeted interventions. With added measurement capabilities and AutoDepth, this all-in-one imaging device* introduces a new frontier in complex wound care scenarios.

.jpg)