
.jpg)
Clinical Research
Assessment of tissue perfusion in the setting of peripheral artery disease (PAD) remains problematic. The ability to assess the need for revascularization or when wound care alone is appropriate as the primary treatment modality is dependent on such an assessment. Current techniques, such as the ankle-brachial index, segmental pressures, transcutaneous oxygen measurements, and skin perfusion pressure, provide limited insight into microvascular perfusion and often fail to reliably predict wound healing. This trial studied near-infrared spectroscopy (NIRS) as a non-invasive method to assess tissue oxygenation thereby improving diagnosis and prognostication in PAD.
Methods:
A prospective study was performed in thirty subjects with varying degrees of PAD. Metrics of tissue perfusion were measured with a non-invasive imaging device utilizing NIRS (SnapshotNIR, Kent Imaging, Calgary, Canada). A comparison was made between NIRS and ABI with stratification by clinical presentation. Two patients were excluded due to missing data, leaving 28 for analysis in three clinical groups: asymptomatic (normal ABI), intermittent claudication (ABI 0.50–0.85), and critical limb ischemia (CLTI, ABI ≤0.49). Plantar and dorsal foot images were captured, and NIRS-derived parameters were determined at standardized locations: oxyhemoglobin (HbO), deoxyhemoglobin (Hb), total hemoglobin (HbTot), and tissue oxygen saturation (StO₂). Multivariate analysis of variance (MANOVA) tested global group differences, followed by univariate ANOVA and post-hoc comparisons. All statistical analyses were performed using SPSS software.
Results:
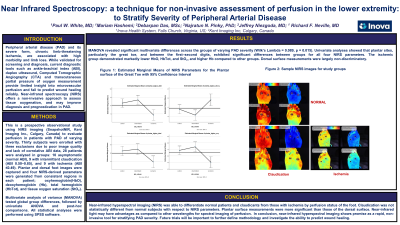
The study cohort consisted of three groups without differences in demographics; 10 asymptomatic, 10 claudication, 8 CLTI. Multivariate analysis (MANOVA) revealed significant differences in perfusion metrics across all groups (Wilk’s Lambda = 0.089, p = 0.015). Univariate analysis showed that plantar sites (great toe, ball of first–second digits) exhibited significant differences for all four NIRS perfusion parameters. There was no significant difference between asymptomatic and claudication, but CLTI demonstrated markedly lower HbO, HbTot, and StO₂, and higher Hb compared to both other groups (p< 0.05). Dorsal measurements were largely non-discriminatory, except for Hb and StO₂ at only one site.
Discussion:
NIRS is a non-invasive technology that can measure physiological aspects of tissue perfusion, and importantly, can differentiate CLTI from asymptomatic PAD and claudication. NIRS-derived metrics may serve as valuable predictors of disease severity and inform clinical decision-making with promise as a rapid, non-invasive tool for stratifying PAD severity and guiding targeted interventions.