
.jpg)
Case Series/Study
Complex wounds such as traumatic soft-tissue injuries, osteomyelitis-associated tunnels, maceration with fungal overgrowth, and contaminated blast wounds present significant barriers to healing due to rapid biofilm reformation, persistent inflammation, and moisture imbalance. Standard modalities including irrigation and cleansing provide known benefits but often result in only temporary improvement and cannot maintain acidic pH that inhibits bacterial growth. This case series evaluates a structured multimodal protocol combining pure hypochlorous-acid* (HOCL), Prontosan* (polyhexamethylene biguanide (PHMB) plus betaine ), and a pH-neutral synergistic ionic silver (0.01%)–menthol liquid (Silverstream*) dressing applied for continuous 24-hour contact.
Methods:
Six patients with acute and chronic complex wounds underwent a three-step wound treatment protocol. Step 1 involved extended HOCL irrigation for at least 30 minutes to reduce surface contamination. HOCL solution has 2.5 pH; neutralizes odors; reduces pain and itching. HOCL is non-toxic for granulation tissue. Step 2 consisted of PHMB plus betain application for an additional 30 minutes to suppress microbial activity, detach deeper debris and break down biofilm, followed by mechanical cleansing. Step 3 involved application of Silverstream solution, which possesses unique properties including biofilm destruction, cleansing, removal of slough, moisture balance and protection of viable tissue. Wet pads soaked in the solution were left in the wounds for 24 hours, deep wounds were packed. All three solutions exhibit broad-spectrum antibacterial activity, effectively target Candida and fungi, and contribute to accelerating the healing process.
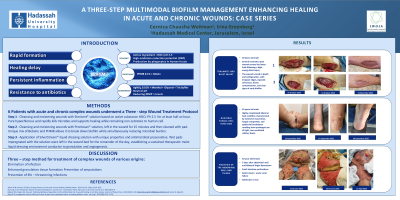
Results:
All wounds showed rapid stabilization and consistent progression toward healing. Traumatic and blast injuries achieved full closure within approximately three weeks. An osteomyelitic tunnel reduced from 16 cm in length to 0.5 cm depth within 25 months. Severe bilateral fungal heel maceration improved markedly within the first 48 to 72 hours and progressed to full restoration of the skin barrier within 17 days. In a case of extensive necrosis of the abdominal wall and thighs after a liposuction procedure, surgical resection was performed with partial improvement and return of fibrin tissue and slough. The three-step treatment over 10 days reduced the fibrin tissue and slough, promoted good granulation tissue, and allowed skin grafting. There were no side effects associated with the three-step wound treatment protocol.
Discussion: The three-step method was subsequently applied to the treatment of complex wounds of various origins. This multimodal protocol promoted elimination of infection, enhanced granulation tissue formation, prevented amputations and life-threatening infections, accelerated recovery, and improved quality of life.