(CR-064) Real-World Use of a Decellularized Porcine Placental Extracellular Matrix in Hard-to-Heal Wounds: A Retrospective, Single-Center Study
Friday, April 10, 2026
Cristin Taylor, PA; Helen Hahn, BSN; Christopher Michaelis, Doctor of Osteopathic Medicine DO
Introduction: Hard-to-heal wounds do not transition through the typical phases of healing in a reasonable time despite appropriate standard of care.1 Cellular, acellular, matrix-like products (CAMPs) have been developed to augment the conventional care of these wounds. Randomized controlled trials and meta-analyses suggest that the addition of these products to standard care of hard-to-heal wounds can improve outcomes over standard care alone.2,3,4 This retrospective, single-center study aimed to collect and evaluate real-world performance data on PPECM*, a novel CAMP produced from decellularized porcine placenta, in the management of hard-to-heal wounds.
Methods: Electronic medical records at a single wound clinic were screened for patients with hard-to-heal wounds, whose care included the use of PPECM* between May 2022 – March 2024. Hard-to-heal wounds were defined as those with < 50% reduction in wound area over 4-weeks of standard treatment. The primary endpoint was wound percent area reduction (PAR) at 4-weeks, with secondary endpoints including PAR at 12- and 20-weeks, and likelihood of wound closure over time.
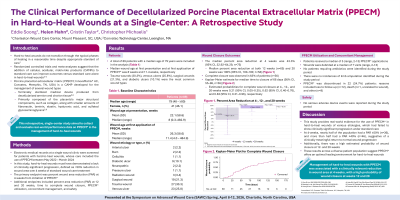
Results: A total of 89 patients with a median age of 79 were included. Trauma wounds (30.3%), venous ulcers (25.8%), surgical wounds (21.3%), and diabetic ulcers (10.1%) were most common. Median wound age at first PPECM* application was 11.4 weeks [IQR: 7.3 – 20.1], and median number of PPECM* applications was 5.0 [min: 2.0, max: 13.0]. The median PAR at 4- and 12-weeks was 43.33% [95% CI: 32.92 – 64.29, n=80] and 100% [95% CI: 100 – 100, n=65]. Wound closure was observed in 63% of subjects (n=56). Kaplan-Meier (KM) estimate for median time to complete wound closure was 66 days [95% CI: 55 – 96, n=56]. KM estimates for probability of wound closure at 4-, 12-, and 20-weeks were 0.21 [95% CI: 0.05 – 0.35], 0.62 [95% CI: 0.40 – 0.76], and 0.83 [95% CI: 0.31 – 0.96].
Discussion: Hard-to-heal wounds managed with PPECM* showed a clinically relevant reduction in wound area at 4 weeks, with a high probability of closure at weeks 12 and 20. PPECM* may provide an optimal environment for healing, supporting the closure of the majority of hard-to-heal wounds.

.jpg)