
.jpg)
Clinical Research
Introduction: Diabetic foot ulcers (DFUs) are the most common complication of diabetes, and have significant impact on morbidity and mortality.1,3 Studies indicate that concurrent lymphedema impairs healing in DFUs.2,3 Peripheral edema, found in 38% of DFUs, has been associated with worse outcomes.2 RCTs have shown that edema management improves outcomes.1 The current IWGDF guidelines advise assessment of edema and treatment of edema when present, no recommendations are provided on intervention.5 Our objective was to compare healing outcomes in individuals with active DFU, lymphedema and concurrent leg ulcer (DFU/LE/LU) versus those with DFU, lymphedema and no concurrent leg ulcer (DFU/LE) treated with and without manual lymphatic drainage (MLD).
Methods:
Materials and Methods: A retrospective cohort study was conducted over a 10-year period at a multidisciplinary wound center. Patients with DFU/LE/LU and DFU/LE were divided into cohorts: those who received MLD and those who did not. Primary outcomes measured were time to complete DFU closure and healing of DFU at 12 weeks and 20 weeks.
Results:
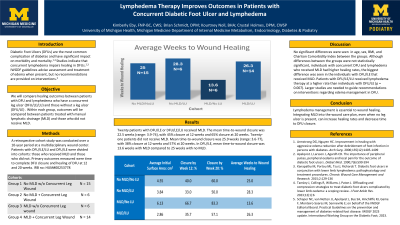
Results: Twenty patients (DFU/LE and DFU/LE/LU) received MLD. The mean-time-to-wound healing was 22.5 weeks (range: 3.9-74). Closure rates were 45% by 12 weeks, 65% by 20 weeks. Twenty-one patients did not receive MLD. The mean-time-to-wound closure was 25.9 weeks (range: 3.6-77). Closure rates were 38% by 12 weeks, 57% by 20 weeks. In DFU/LE, mean-time-to-wound closure for MLD cohort was 13.6 weeks compared to 25 weeks in no MLD cohort.
Discussion:
Discussion: Although differences between the groups were not statistically significant, individuals with concurrent DFU and lymphedema who received MLD had higher healing rates, the biggest difference was seen in the individuals with DFU/LE that received MLD. Patients with DFU/LE/LU received lymphedema therapy at a higher rate than individuals with DFU/LE (p = 0.007). Larger studies are needed to confirm the impact of lymphedema therapy on DFU outcomes and guide recommendations on interventions regarding edema management in DFU.