(CS-091) Use of a Borate-Based Bioactive Glass Fiber Matrix in the Treatment of Complex Lower Extremity Wounds: A Case Series
Friday, April 10, 2026
Introduction: Chronic and complex wounds of the lower extremities are often refractory to standard care, particularly when complicated by infection, ischemia, or systemic comorbidities. Bioactive glass materials, such as borate-based bioactive glass, have gained interest for their ability to provide an extracellular like matrix environment that may facilitate angiogenesis and tissue regeneration.1-4 This case series evaluates the effectiveness of a borate-based bioactive glass fibrous matrix (BBGFM) in treating four complex wounds, using percent area reduction (PAR) as the primary outcome
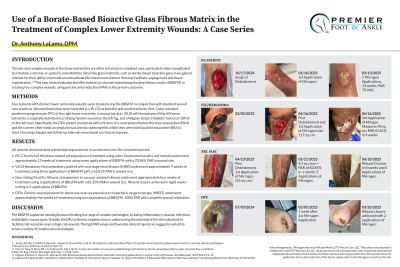
Methods: Four patients with distinct lower extremity wounds were treated using the BBGFM in conjunction with standard wound care practices. Wound dimensions were recorded (L x W x D) at baseline and monitored over time. Cases included: pyoderma gangrenosum (PG) of the right lower extremity, a venous leg ulcer (VLU) with hematoma of the left lower extremity, a surgically debrided necrotizing fasciitis wound on the left leg, and a Wagner Grade 3 diabetic foot ulcer (DFU) on the left heel. Specifically, the DFU patient presented with a history of a contralateral below the knee amputation (BKA) and the current chief medical complaint was chronic osteomyelitis which they were told would need another BKA to treat. Dressing changes and follow-up.
Results: All wounds demonstrated substantial improvement in wound area over the treatment period: • PG: Chronic full-thickness wound unresponsive to treatment using ovine forestomach matrix and morsels underwent approximately 13 weeks of treatment using seven applications of BBGFM with a 70.96% PAR in wound size. • VLU/Hematoma: Non ambulatory patient with end stage renal disease (ESRD) underwent approximately 9 weeks of treatment using three applications of BBGFM with a 65.81% PAR in wound size. • Necrotizing Fasciitis: Wound unresponsive to vacuum-assisted closure underwent approximately four weeks of treatment using 3 applications of BBGFM with a 83.35% PAR in wound size. Wound closure achieved in eight weeks ending in 5 applications of BBGFM. • DFU: Chronic wound present for about one year unresponsive to hyperbaric oxygen therapy (HBOT) underwent approximately five weeks of treatment using two applications of BBGFM, 100% PAR with complete wound resolution.
Discussion: The BBGFM supported meaningful wound healing in a range of complex pathologies, including inflammatory, vascular, infectious, and diabetic wound types. Notably, the DFU achieved complete closure, underscoring the potential of this skin substitute to facilitate full resolution even in high-risk wounds. The high PAR values and favorable clinical trajectories suggest broad utility across a variety of complex wound etiologies.

.jpg)