(CS-150) Adjunctive Borate-Based Bioactive Glass Fiber Matrix (BBGFM) Therapy Enhances Granulation and Closure in Chronic Diabetic Foot Ulcers
Friday, April 10, 2026
Scott Littrell, DPM
Introduction: Diabetic foot ulcers (DFUs) remain a major clinical challenge due to impaired perfusion, chronic inflammation, and high susceptibility to infection.1,2 Advanced biologically active matrices have emerged as adjunctive therapies to support wound bed preparation and progression toward closure. Randomized controlled trials have reported improved wound healing trajectories and high rates of wound closure when BBGFM is integrated into standard diabetic foot care protocols, highlighting its potential to accelerate wound resolution and reduce downstream complications.1,2 Building on this emerging evidence, we conducted a clinical case series evaluating BBGFM in real-world patients with complex DFUs receiving guideline-based care.
Methods: Seven patients with DFUs of varying size, duration, and complexity were followed. All participants continued standard wound management including moisture balance, offloading or compression, debridement as indicated, and scheduled follow-up. BBGFM was applied and wound area was measured at baseline and weekly thereafter until closure or substantial improvement. Clinical observations, infection control, suitability for surgical intervention, and progression to advanced therapies (e.g., wound vacuum assisted closure (VAC)) were documented.
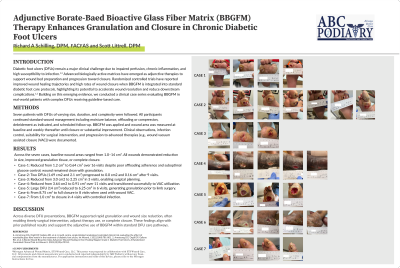
Results: Across the seven cases, baseline wound areas ranged from 1.0–14 cm². All wounds demonstrated reduction in size, improved granulation tissue, or complete closure. • Case-1: Reduced from 1.2 cm² to 0.64 cm² over 16 visits despite poor offloading adherence and suboptimal glucose control; wound remained clean with granulation. • Case-2: Two DFUs (1.69 cm2 and 2.1 cm²) progressed to 0.0 cm2 and 0.16 cm² after 9 visits. • Case-3: Reduced from 3.0 cm2 to 2.25 cm² in 3 visits, enabling surgical planning. • Case-4: Reduced from 3.64 cm2 to 0.91 cm² over 11 visits and transitioned successfully to VAC utilization. • Case-5: Large DFU (14 cm²) reduced to 6.25 cm² in 6 visits, generating granulation prior to limb surgery. • Case-6: From 8.75 cm² to full closure in 8 visits when used with wound VAC. • Case-7: From 1.0 cm² to closure in 4 visits with controlled infection.
Discussion: Across diverse DFU presentations, BBGFM supported rapid granulation and wound size reduction, often enabling timely surgical intervention, adjunct therapy use, or complete closure. These findings align with prior published results and support the adjunctive use of BBGFM within standard DFU care pathways.

.jpg)