(CR-020) Enhanced silver dressing versus dialkylcarbamoyl chloride-coated dressing in venous leg ulcers: a blinded re-assessment of randomized controlled trial findings
Friday, April 10, 2026
Constanza Cabrera, MD – Convacare Clinics, Bogotá, Colombia; Jan Ljungqvist, BSc – Convatec Technology Centre, Deeside, United Kingdom; Rebecca Rodger, BSc – Convatec Technology Centre, Deeside, United Kingdom; Beate Paintner-Hanson, MD – Convatec Technology Centre, Deeside, United Kingdom
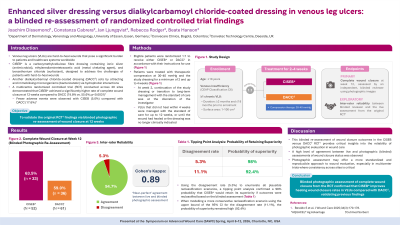
Introduction: Venous leg ulcers (VLUs) are hard-to-heal wounds that pose a significant burden to patients and healthcare systems worldwide. A carboxymethylcellulose fibre dressing containing ionic silver, ethylenediaminetetraacetic acid, and benzethonium chloride (CISEB*) was designed to address the challenges of patients with hard-to-heal wounds. A previous randomized controlled trial (RCT) demonstrated a significantly higher rate of complete wound closure at 12 weeks with CISEB compared to a dialkylcarbamoyl chloride-coated dressing (DACC†; 74.8% vs. 55.6%, p< 0.0031).1 The current study aimed to validate these findings through an independent, blinded re-assessment of wound closure status.
Methods: Patients with hard-to-heal VLUs were randomized 1:1 to receive either CISEB or DACC for ≤4 weeks. Wounds not healed by week 4 were subsequently managed with standard of care for ≤12 weeks or until healed. The complete study design has been previously described.1 The primary endpoint was incidence of complete wound closure at week 12, assessed by an independent, blinded reviewer using photographs. Inter-rater reliability was an exploratory endpoint. A post hoc tipping analysis modeled the probability of outcome reclassification based on disagreement rates.
Results: A total of 113 VLUs from 105 patients were included (CISEB: n=49; DACC: n=56). Agreement between the independent reviewer and the original RCT assessment was 94.7%, with a Cohen’s Kappa of 0.89, indicating ‘near-perfect’ agreement. Using the disagreement rate (5.3%) to enumerate all plausible reclassification scenarios, the tipping point analysis confirmed a 98% probability CISEB would retain its superiority if outcomes were reclassified based on the blinded assessment. When modelling a more conservative reclassification scenario using the upper bound of the 95% CI for the disagreement rate (11.1%), the probability of superiority remained high at 92.4%. High inter-rater agreement was generally observed across countries and study sites. By week 12, CISEB was associated with a higher rate of complete wound closure compared to DACC (63.5% vs. 59.0%).
Discussion: The strong inter-rater reliability supports the robustness of the results and reinforces the role of CISEB as a standard of care for managing hard-to-heal VLUs. Independent blinded assessment confirmed that CISEB improves wound closure rates in hard-to-heal VLUs compared to DACC, aligning with previous RCT findings.

.jpg)