
.jpg)
Health Economics
Prior research indicates that use of the PHMB antimicrobial wound matrix (“PCMP*”) is frequently delayed until individuals develop more severe diabetic foot ulcers (“DFUs”). This study evaluated rates of non-traumatic lower-limb amputations (“amputations”) among beneficiaries with DFUs who initiated PCMP within 6 months of diagnosis compared with those who never receiving PCMP.
Methods:
Two mutually exclusive cohorts of beneficiaries with DFUs were identified from 100% Medicare Fee-for-Service Standard Analytic Files (Q1 2015–Q3 2023): (i) those receiving PCMP within 6 months of DFU diagnosis (first PCMP claim defined as the index date) and (ii) those receiving standard wound care (e.g., debridement, offloading) without PCMP (index date randomly assigned). Beneficiaries were matched 1:1 and required to have continuous Medicare Parts A and B enrollment for ≥6 months pre- and post-index. Six-month post-index amputation rates were compared using statistical tests for matched pairs. Additionally, amputation rates among beneficiaries initiating PCMP within 45, 60, or 90 days of diagnosis—and receiving follow-up applications every 7–14 days for one month—were descriptively compared with rates among those never receiving PCMP. Standardized mean differences (SMD) >10% and p-values < 0.05 were considered statistically significant.
Results:
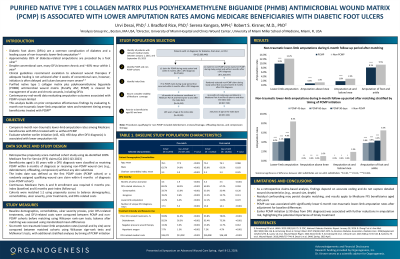
Before matching, beneficiaries receiving PCMP (N=10,939) had greater disease severity, as indicated by longer duration of active ulceration and higher amputation rates in the 6 months pre-index than those never treated with PCMP (N=657,233). Post-matching, baseline differences were eliminated. During the 6-month follow-up period, beneficiaries receiving PCMP (N=10,862) had lower amputation rates than matched controls (9.9% vs. 12.2%; SMD=–7.34%; p< 0.001). Further, among beneficiaries initiating PCMP within 45, 60, or 90 days of diagnosis (N=506; 684; 946), 6-month amputation rates were 4.0%, 4.1%, and 4.8%, respectively, compared with 8.4% among non-PCMP recipients (all p< 0.001).
Discussion:
Findings from this study reaffirm that PCMP treatment is often delayed until DFUs become more severe. However, after adjusting for baseline differences, PCMP use was associated with lower rates of non-traumatic lower-limb amputations during the 6-month follow-up period. Earlier initiation—particularly within 90 days of DFU diagnosis—may further reduce amputation risk.