(CS-031) A Bordered Silicone Foam Dressing as Secondary Coverage Over Collagen-Based Primary Treatments in Chronic Full-Thickness Pressure Injuries: A Prospective Case Series
Friday, April 10, 2026
Nirman Tulsyan, MD FACS RPVI – President, Heritage Wound Care
Introduction: Chronic full-thickness pressure injuries (PIs) open beyond 90 days often demonstrate stalled healing despite advanced primary treatments. Collagen-based primary treatments—ranging from collagen dressings to cellular tissue-based products (CTPs) and platelet-rich plasma (PRP)—stimulate extracellular matrix deposition but require effective secondary coverage to manage exudate and protect developing tissue. Recent Medicare coverage policy changes for CTPs and Coverage with Evidence Development requirements for PRP have created variable access to advanced therapies across clinical settings. Clinicians need versatile secondary dressings that perform consistently regardless of which collagen-based primary treatment is accessible. This prospective case series evaluates a three-dimensional conforming bordered silicone foam dressing* as secondary coverage over various collagen-based primaries in chronic PIs with depths of 0.5-2.0 cm.
Methods: Ten patients with PIs open >90 days were enrolled. Baseline assessments included wound depth, tissue type, periwound condition, pain scores, and subcutaneous perfusion using infrared thermography†. Collagen-based primary treatments were applied to debrided wound beds, followed by the bordered silicone foam dressing* as secondary coverage. Dressing changes occurred three times weekly. Weekly assessments documented wound depth, granulation tissue formation, periwound status, wound bed temperature, patient-reported pain, dressing adherence, and wear time over six weeks.
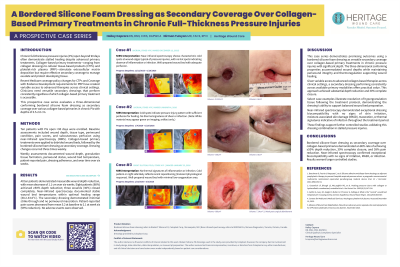
Results: All ten patients demonstrated measurable wound depth reduction, with mean decrease of 1.1 cm over six weeks. Eight patients (80%) achieved ≥50% depth reduction; three wounds (30%) closed completely. Infrared thermography† documented stable wound bed temperatures within optimal healing range (30.2-33.0°C). The secondary dressing demonstrated minimal strike-through and no periwound maceration. Patient-reported pain scores decreased from mean 5.2 at baseline to 2.1 at week six (59% reduction). No adverse events were observed.
Discussion: This case series demonstrates promising outcomes using a bordered silicone foam dressing as versatile secondary coverage over collagen-based primary treatments in PIs with significant depth. The three-dimensional conforming properties accommodated wound depths while maintaining periwound integrity and thermoregulation supporting wound healing. Given variable access to advanced collagen-based therapies across clinical settings, a secondary dressing performing consistently across available primary modalities offers practical value. This approach achieved substantial depth reduction and 30% complete closure. These findings support further controlled studies validating this dressing combination in stalled PIs.

.jpg)