(CS-142) A complex case study showing the use of biodegradable bilayer synthetic matrix in the treatment of necrotizing fasciitis of the forearm and hand
Friday, April 10, 2026
Mahmoud Hassouba, MD, PhD; David Hill, PharmD, BCPS, BCCCP, FCCM; Mahnoush Mohmeni, MD
Introduction: Necrotizing fasciitis, a soft tissue infection, travels along the fascial plane, causing secondary infection of surrounding tissue (1). Skin breakdown, accompanied by bullae and cutaneous gangrene, can progress to sepsis. Treatment involves empiric antibiotics, an aggressive surgical approach, and adjustment of antimicrobial coverage to identified pathogens (1).
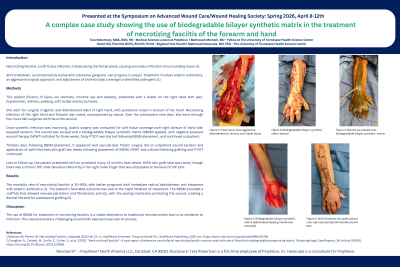
Methods: This patient [history of lupus (on steroids), nicotine use and obesity], presented with a blister on the right hand with pain, hypotension, redness, swelling, with bullae and ecchymoses. She went for surgical irrigation and debridement (I&D) of right hand, with purulence noted in dorsum of her hand. Necrotizing infection of the right hand and forearm was noted, accompanied by sepsis. Over the subsequent nine days, she went through four more I&D surgeries with the ortho service. Once systemic infection was improving, plastic surgery was consulted for soft tissue coverage over right dorsum of hand with exposed tendons. The wound was excised and a biodegradable bilayer synthetic matrix (BBSM) applied, with negative pressure wound therapy (NPWT) initiated for three weeks. Daily PT/OT was started following BBSM placement, and continued outpatient. Thirteen days following BBSM placement, it appeared well vascularized. Plastic surgery did an outpatient wound excision and application of split-thickness skin graft ten weeks following placement of BBSM. NPWT was utilized following grafting and PT/OT continued. Lost to follow-up, the patient presented with an unrelated injury 13 months later where 100% skin graft take was noted, though there was a chronic DIP ulnar deviation deformity in her right index finger that was amputated at the level of DIP joint.
Results: The mortality rate of necrotizing fasciitis is 30-90%, with better prognosis with immediate radical debridement and treatment with empiric antibiotics (1). This patient’s favorable outcome was due to the rapid initiation of treatment. The BBSM provided a scaffold that allowed neovascularization and fibroblastic activity, with the sealing membrane protecting the wound, creating a dermal-like bed for subsequent grafting (2).
Discussion: The use of BBSM for treatment of necrotizing fasciitis is a viable alternative to traditional reconstruction due to its resilience to infection. This case presented a challenging wound with exposed avascular structures.

.jpg)