(CS-074) Use of a Borate-Based Bioactive Glass Fiber Matrix in the Management of a Complex Stage 4 Pressure Injury in a Patient With Paraplegia: A Case Report
Friday, April 10, 2026
Introduction: Stage 4 pressure injuries (PIs) in individuals with spinal cord injury remain among the most challenging chronic wounds to manage. These wounds often demonstrate prolonged healing trajectories due to underlying immobility, recurrent mechanical stress, and the presence of deep tissue destruction. Patients with paraplegia are particularly susceptible to recurrent and complex ulcerations, frequently requiring multimodal interventions and prolonged inpatient care.1 Advanced wound matrices, including a Borate-Based Bioactive Glass Fiber Matrix (BBGFM), have emerged as adjunctive options when standard wound care alone results in delayed progression. This case report describes the clinical course of a large stage 4 PI that demonstrated substantial improvement following introduction of BBGFM in conjunction with negative-pressure wound therapy (NPWT).
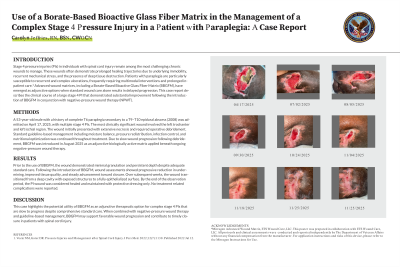
Methods: A 53-year-old male with a history of complete T6 paraplegia secondary to a T9–T10 epidural abscess (2008) was admitted on April 17, 2025, with multiple stage 4 PIs. The most clinically significant wound involved the left trochanter and left ischial region. The wound initially presented with extensive necrosis and required operative debridement. Standard guideline-based management including moisture balance, pressure redistribution, infection control, and nutritional optimization was continued throughout treatment. Due to slow wound progression following debridement, BBGFM was introduced in August 2025 as an adjunctive biologically active matrix applied beneath ongoing negative-pressure wound therapy.
Results: Prior to the use of BBGFM, the wound demonstrated minimal granulation and persistent depth despite adequate standard care. Following introduction of BBGFM, wound assessments showed progressive reduction in undermining, improved tissue quality, and steady advancement toward closure. Over subsequent weeks, the wound transitioned from a deep cavity with exposed structures to a fully epithelialized surface. By the end of the observation period, the PI wound was considered healed and maintained with protective dressing only. No treatment related complications were reported.
Discussion: This case highlights the potential utility of BBGFM as an adjunctive therapeutic option for complex stage 4 PIs that are slow to progress despite comprehensive standard care. When combined with negative-pressure wound therapy and guideline-based management, BBGFM may support favorable wound progression and contribute to timely closure in patients with spinal cord injury.

.jpg)