
.jpg)
Evidence-Based Practice
Hard-to-heal wounds impose substantial morbidity, cost, and, in the case of diabetic foot ulcers, elevated
mortality risk. Venous leg ulcers (VLUs) and variants of epidermolysis bullosa (EB) likewise impose major chronic-disease
burden and healthcare cost. Keratin biomaterials
Methods:
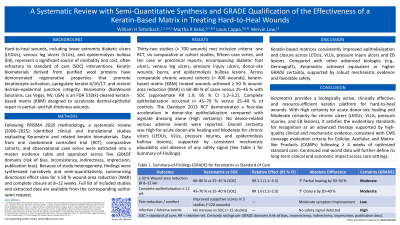
Literature from 2006–2025, including a randomized controlled trial (RCT), prospective cohorts, and case-series
data, was extracted into a master evidence table. Studies were assessed in accordance with the Preferred Reporting Items
for Systematic Reviews and Meta-Analyses (PRISMA 2020) and evaluated across five GRADE domains with appropriate
downgrading and upgrading factors. Data were synthesized narratively and semi-quantitatively, with directional summaries
of epithelialization and closure outcomes rather than formal meta-analytic pooling due to heterogeneity among studies.
Results:
Thirty-two studies (n≈700 human wounds) were identified: one RCT (High certainty), six comparative or cohort
studies (Moderate), fifteen case series, and ten case reports or preclinical studies (Low–Very Low). Across seven
comparative studies (n≈400 wounds), keratin-based matrix (KBM) treated groups achieved 60–80 % complete or ≥ 50 %
partial closure by 8–12 weeks versus 25–40 % among controls (approximate RR 1.97; 95 % CI 1.2–3.2). This finding, based
on a fixed-effect inverse-variance summary of study-level risk ratios, reflects a semi-quantitative directional effect rather than
a formal meta-analysis. Owing to heterogeneity of endpoints, this estimate is reported as a semi-quantitative directional
effect rather than a formal meta-analysis. Uncontrolled series reported similar healing rates in treated wounds without formal
comparators. No serious adverse events were reported.
Discussion:
Using formal GRADE qualification, the KBM used in these studies demonstrate consistent clinical efficacy and
favorable safety across diabetic foot ulcers, venous leg ulcers, and epidermolysis bullosa. Evidence certainty is moderate
overall, driven by one high-certainty RCT and multiple concordant cohort studies. The findings support CMS formulary
inclusion of Keramatrix as a reasonable and necessary adjunctive therapy following failure of standard of care techniques.
Ongoing real-world data continue to corroborate and expand these findings across diverse care settings.