
.jpg)
Case Series/Study
Patients who have undergone massive weight loss (MWL) face unique surgical recovery challenges due to significant redundant skin and subcutaneous tissue laxity. Research indicates that seroma formation risk increases substantially with the volume of tissue removed in this population.1 While small seromas may resolve spontaneously, chronic seromas often develop a fibrous pseudocapsule (pseudobursa) that prevents fluid reabsorption.2,3 This report details the surgical management of a complex, recurrent chronic seroma in the thigh of an MWL patient following total hip arthroplasty (THA).
Methods:
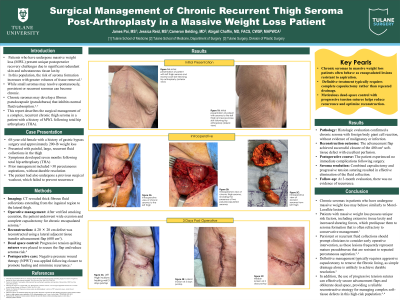
A 68-year-old female with a history of gastric bypass and 200-lb weight loss presented with painful, large, recurrent fluid collections seven months after her initial THA. The patient had failed over 30 percutaneous aspirations and a previous surgical washout. CT imaging revealed thick, fibrous collections extending from the inguinal region to the lateral thigh. Following verified smoking cessation, the patient underwent wide excision of the masses and total capsulectomy, a technique indicated for chronic encapsulated lesions.3 The resulting 20x20cm lateral defect was reconstructed using a 600 cm² lateral adjacent tissue transfer advancement flap. Progressive tension quilting sutures were utilized to obliterate dead space and fixate the flap, a method proven to significantly reduce seroma rates compared to drains.4 Negative pressure wound therapy (NPWT)* was applied post-closure to further promote granulation and reduce recurrence.3
Results:
Pathology confirmed the diagnosis of a chronic seroma with a foreign body giant cell response, negative for malignancy or infection. The advancement flap successfully closed the large 400 cm² tissue defect, demonstrating excellent perfusion. The patient experienced no immediate post-operative complications, and the combination of capsulectomy and tension sutures effectively resolved the fluid collection. At 3 month follow-up, there was no recurrence
Discussion:
Chronic seromas in MWL patients behave similarly to Morel-Lavallée lesions, where a fibrous lining prevents fluid resorption and creates a permanent potential space. Patients with massive weight loss possess unique risk factors – specifically extensive tissue laxity and shearing forces – that predispose them to seroma formation refractory to conservative management.1 Clinicians should maintain a low threshold for converting from conservative management to surgical excision when fluid collections persist, as these often represent mature pseudobursas resistant to percutaneous aspiration.2,3 This case demonstrates that resolution requires aggressive capsulectomy to remove the fibrotic lining, rather than simple drainage.3 Furthermore, the use of progressive tension sutures effectively anchors the flap and obliterates dead space, offering a reliable solution for complex defects in this high-risk population.4,6