
.jpg)
Clinical Research
Diabetic foot ulcers (DFUs) commonly exhibit prolonged, nonhealing trajectories, contributing to substantial morbidity, increased mortality risk, and considerable financial burden. Standard-of-care (SOC) often results in dissatisfactory outcomes, demanding a need for advanced, cost-efficient interventions capable of improving wound closure rates in hard to heal ulcers.
Methods:
An interim analysis of this multicenter, prospective, randomized, controlled, modified platform trial evaluated efficacy of multiple cellular, acellular, and matrix-like products (CAMPs) plus SOC versus SOC alone. The primary objective was to determine the proportion of DFUs achieving complete closure in 12 weeks. Secondary assessments included percentage area reduction (PAR).
Results:
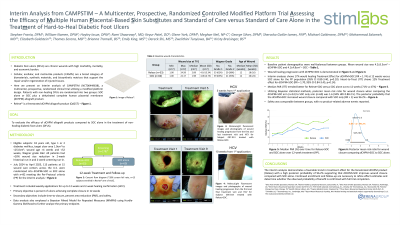
Baseline demographics and clinical characteristics were similar between groups. In Intent-To-Treat (ITT), the fenestrated dehydrated complete human placental membrane* (dCHPM) allograft plus SOC arm (n=53) yielded an 11.6% absolute gain in wound closure rate treatment effect vs. SOC alone (n=60) (95% confidence interval (CI) [-3.7%, 26.8%], p=0.14). In Per Protocol (PP), the dCHPM plus SOC arm (n=38) demonstrated a 16.8% absolute gain in wound closure rate treatment effect vs. SOC alone (n=44), trending towards significance (95% CI [-3.2%, 35.4%], p = 0.10). Relative risk analysis further supported a favorable effect in complete closure: dCHPM plus SOC increased the likelihood of complete closure by 1.70 (95% CI [0.84, 3.45]) in ITT and by 1.74 (95% CI [0.89, 3.40]) in PP. This corresponds to 70% (ITT) and 74% (PP) higher relative closure probabilities compared to SOC alone. Percent area reduction (PAR, cm2) over 12 weeks was also analyzed. For ITT and PP, dCHPM plus SOC outperformed SOC alone (ITT; median SOC: 47.1%, dCHPM: 71.1%). Safety outcomes were similar between groups, and no product-related adverse events were reported.
Discussion:
Interim findings indicate that dCHPM allografts provide a favorable treatment effect in wound closure trajectories. The consistent trends in closure rate, PAR, and safety support continued trial enrollment, with the expectation that full study completion will more definitively characterize treatment benefit.