
.jpg)
Case Series/Study
Excessive bacterial burden, particularly levels surpassing the chronic inhibitory bacterial load (CIBL) of approximately 10⁴ CFU/g, is strongly associated with stalled closure in chronic wounds such as diabetic foot ulcers (DFUs). Fluorescence imaging has emerged as a practical method to visualize these elevated bacterial concentrations in the wound bed and surrounding skin. Conventional management, which often relies on sharp debridement supported by topical antiseptics, may require multiple weeks to reduce fluorescence and generally does not address microbial activity in the periwound region. A topical desiccating agent (TDA1), formulated to dehydrate tissue, disrupt biofilm matrices, and rapidly kill bacteria while sparing intact skin, has been proposed as an alternative debridement modality. This case series evaluates the effect of a single TDA application on bacterial load indicators and early healing progression in DFUs.
Methods:
Fourteen individuals with chronic DFUs underwent chemical debridement with TDA in addition to standard wound care protocols. Clinical follow-up focused on wound appearance, granulation tissue formation, and reduction of fluorescence signals in both the wound bed and periwound skin. No additional applications of TDA were used.
Results:
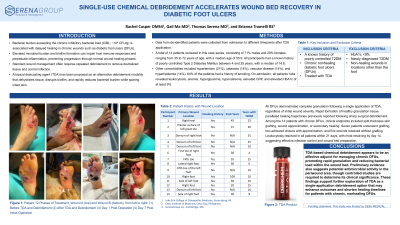
All DFUs demonstrated complete granulation after one application of TDA, regardless of initial wound severity. The rapid formation of healthy granulation tissue paralleled previously reported healing trajectories following sharp surgical debridement. Notably, most wounds exhibited a marked decline in fluorescence intensity, suggesting a substantial reduction in bacterial burden. Qualitative observation also indicated improvements in periwound fluorescence, a region typically unaffected by surgical debridement alone.
Discussion:
TDA-based chemical debridement appears to be an effective adjunct for managing chronic DFUs, promoting rapid granulation and reducing bacterial load within the wound bed. Preliminary evidence also suggests potential antimicrobial activity in the periwound area, though controlled studies are required to determine its clinical significance. These findings support further exploration of TDA as a single-application debridement option that may enhance outcomes and shorten healing timelines for patients with chronic, nonhealing DFUs.