George Wilbanks, MS1 – Donald and Barbara Zucker School of Medicine at Hofstra/Northwell; Edward Li, MS1 – Donald and Barbara Zucker School of Medicine at Hofstra/Northwell; Emily Ronan, MS2 – Donald and Barbara Zucker School of Medicine at Hofstra/Northwell; Kadir Ozler, MS2 – Donald and Barbara Zucker School of Medicine at Hofstra/Northwell; Priscillia Lee, MS2 – Donald and Barbara Zucker School of Medicine at Hofstra/Northwell; James Kim, MS2 – Donald and Barbara Zucker School of Medicine at Hofstra/Northwell; Christina Del Pin, MD – Northwell Health; Marisa Ranire-Maguire, MD – Northwell Health; Alisha Oropallo, MD – Northwell Health
Introduction: Telehealth has become integral to wound management, yet validated tools to triage wound severity remotely remain limited. The Telehealth Wound Severity Scale (TeWSs) was developed to provide structured, decision-support for clinicians during virtual wound assessments. We aimed to evaluate the predictive performance of TeWSs for determining the need for in-person care and to identify optimal cutoff points for clinical triage
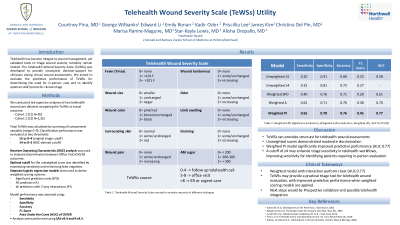
Methods: We conducted retrospective analyses of two telehealth wound care datasets (N=951 and N=1,351). TeWSs is a composite score ranging from 0–9 derived from wound characteristics and systemic indicators, including wound size and appearance, surrounding skin changes, pain, tenderness, swelling, drainage, odor, fever, and glycemic status. Scores were clinically interpreted as continued telehealth follow-up (0–4), office visit (5–8), or emergency/urgent care (≥8), with the primary outcome dichotomized as Office Visit/Emergency–Urgent Care (OV/ER) versus Continued Care/Wound Healed (CC/WH). Total scores were calculated by summing item-level indicators; partially missing items were scored as zero, while fully missing totals were excluded. Predictive performance was assessed using receiver operating characteristic (ROC) analysis and logistic regression–derived weighted scoring models (with and without two-way interactions). Model performance was evaluated using sensitivity, specificity, accuracy, F1 score, and area under the curve (AUC).
Results: Across both datasets, the unweighted TeWSs demonstrated modest discrimination for predicting OV/ER disposition (AUC 0.63 and 0.58). ROC analysis identified a consistent optimal unweighted cutoff of ≥4. Compared with the traditional threshold of ≥5, a cutoff of ≥4 improved sensitivity (0.45 and 0.32), whereas ≥5 favored specificity (0.92 and 0.91) and overall accuracy (0.85 and 0.80). Weighted logistic models improved classification performance. The model incorporating all predictors with two-way interactions achieved the strongest performance across both cohorts (AUC 0.77), with balanced sensitivity (0.53 and 0.65), acceptable specificity (0.87 and 0.78), and the highest F1 scores (0.39 and 0.45)
Discussion: TeWSs provides structure for telehealth wound assessments but offers moderate discrimination when used as an unweighted score. Performance improves markedly with weighted models incorporating all predictors and interactions, indicating important contributions from variable interactions in wound severity assessment. A cutoff of ≥4 may enhance triage sensitivity in telehealth workflows. These findings support further refinement and prospective validation of TeWSs as a telehealth triage tool in wound care.

.jpg)