
.jpg)
Laboratory Research
Negative pressure wound therapy (NPWT) systems are widely used in clinical practice to support healing of surgical incisions, acute and chronic wounds.1 Their clinical effectiveness depends on the system’s ability to consistently deliver the intended negative pressure and manage wound exudate throughout the intended duration of therapy. If pressure delivery or fluid handling is compromised, wound healing may be impaired, increasing the risk of complications.2 In this study, the pressure distribution and fluid management of single-use (su) NPWT systems, designed with or without a canister, is evaluated under simulated clinical use.
Methods:
Three marketed suNPWT systems with multilayer absorptive (MLA) dressing were evaluated: two canister-less systems delivering -80 mmHg, and one canister-based system delivering -125 mmHg. The wound model simulated a moderately exudating wound, using horse serum to mimic wound fluid (viscosity, osmolarity, pH) at a flow rate of 1.1 g/cm²/24 hours and 72 hours dressing-change regimen, according to intended use of the systems. Delivery of the intended negative pressure from the suNPWT pump and its distribution to the simulated wound bed was measured at multiple positions in the model using differential pressure transmitter sensors, sampling data every 60 seconds throughout the test time.
Results:
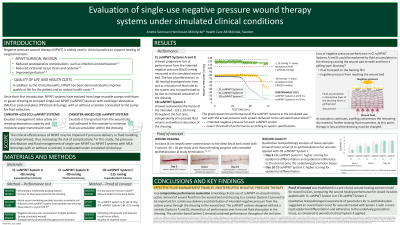
The canister-less systems showed impaired pressure delivery to the wound bed as dressing saturation increased, deviating from the intended -80 mmHg target already after 36 and 50 hours, respectively, and did not recovery during the intended test time. In contrast, the canister-based system maintained consistent pressure delivery at-125 mmHg throughout the test period, unaffected by fluid volume, with no dressing saturation observed.
Discussion: This study demonstrates that the design of the NPWT system significantly affects the ability of suNPWT systems to maintain the intended therapeutic pressure and manage exudate. Limitations in performance, as for the canister-less suNPWT systems, is rationalized to be a consequence of having the dressing as the sole capacity to managing fluid. The canister-based system, with capacity to transport excess exudate and infectious material from the dressing to the canister thereby reducing the risk of dressing saturation, demonstrated superior performance under simulated clinical conditions, suggesting greater reliability in supporting wound healing.